A Case of Renal Hydatid Cyst in a 55-Year-Old Female
A B S T R A C T
The hydatid cyst is a frequent pathology in India. Liver is commonly involved (65%) followed by lungs (25%); muscles (5%); bones (3%) [1]. However, renal hydatid cyst is still rare. It constitutes about 2.5 % of all localizations. It may create diagnostic dilemma at times. We describe a 55-year-old female with left renal hydatid disease managed with enucleation of cyst with nephron sparing surgery (NSS).
Keywords
Hydatid cyst, enucleation, nephron sparing surgery, albendazole
Introduction
Echinococcus granulosus is a cestode (tapeworm) that causes cystic echinococcosis. Infection results from ingestion of food or water contaminated with Echinococcus eggs or contact with infected dogs. Prevalence is high in pastoral communities, particularly in South America, the Mediterranean littoral, Eastern Europe, the Middle East, East Africa, Central Asia, China, Russia, and Australia. After infection the parasites encyst, usually in the liver or (less commonly) in the lungs. Although rare, cysts can grow ectopically in almost any organ in the body, with the kidneys being rare involvement [2].
Case History
55-year-old female presented to OPD with mild discomfort in left lumbar region for 6 months. However, there was no history of severe pain, radiation of pain, nausea, vomiting, burning micturition, or fever. There was no history of hematuria and significant surgical and medical history. Patient had occasional intake of nonveg food. Her general physical examination was normal. Per-abdominal examination was normal, and no lump was palpable. Digital rectal examination and other systemic examination were essentially normal.
Patient underwent USG of Abdomen and CT scan of Abdomen (Figure 1) which were suggestive of ‘exophytic non-enhancing lesion at lower pole of left kidney likely benign etiology possibly Hydatid cyst.’ No similar lesion in contralateral kidney, liver and lungs. Patient was given Tablet Albendazole (400 mg) twice a day for 1 month. Based on large size of the cyst, surgical intervention was planned through open approach. On exploration, a cystic lesion was found over lower pole of left kidney (Figure 2). Mops soaked in sterile savlon solution (cetrimide + chlorhexidine) were spread around kidney to prevent spillage. Cyst was loosely adhered to surround structures and was carefully dissected by blunt and sharp dissection. Ureter was identified. Cyst was excised with rim of normal parenchyma without any spillage (Figure 3). No injury happened to surrounding ureter or renal vessels. Haemostasis was confirmed, retroperitoneal drain was kept and closure was done. Postoperative recovery was uneventful. Patient was given Tablet Albendazole (400 mg) twice a day for 1 month. HPE examination confirmed diagnosis of Hydatid cyst.
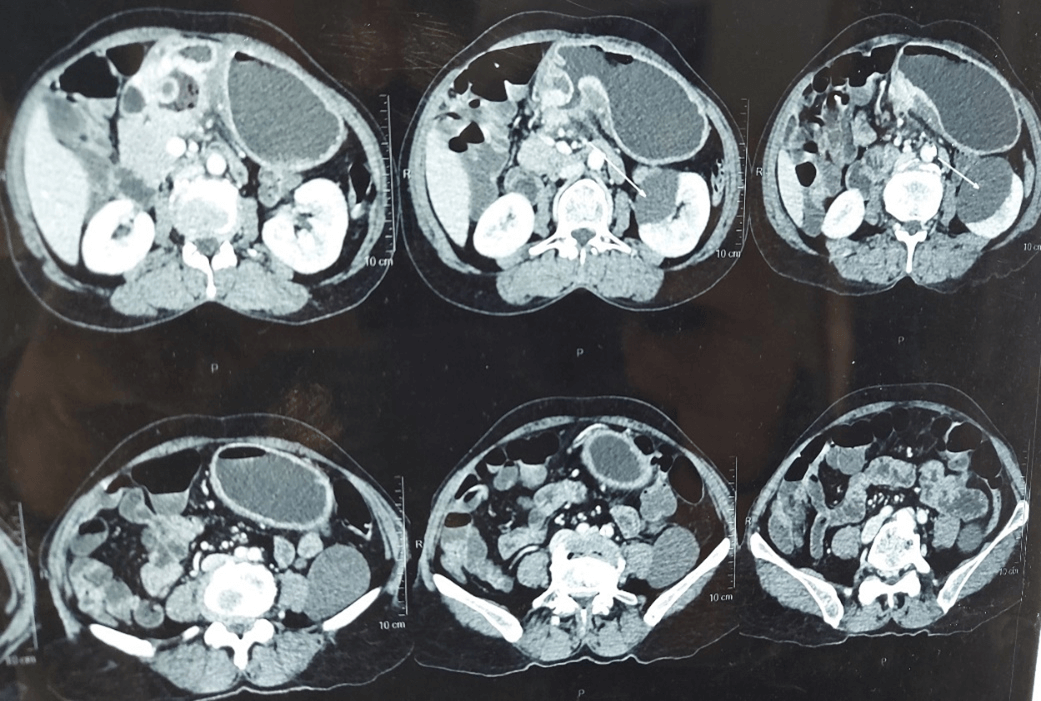
Figure 1: CT scan showing left renal cyst.
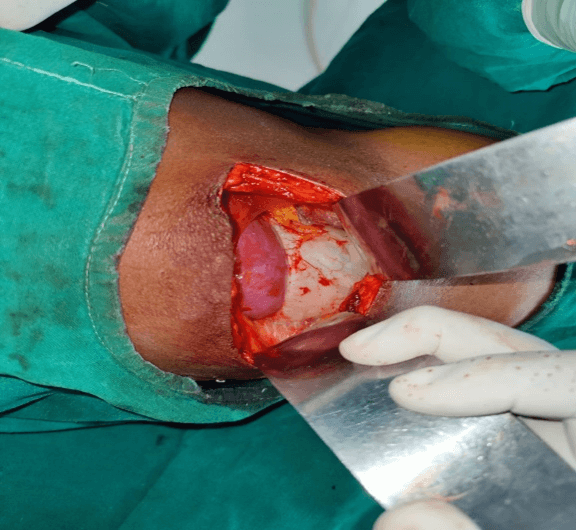
Figure 2: Intraoperative photo.

Figure 3: Size of Cyst.
Discussion
Echinococcus granulosus is a cestode (tapeworm) that causes cystic echinococcosis. Infection results from ingestion of food or water contaminated with Echinococcus eggs or contact with infected dogs. Prevalence is high in pastoral communities, particularly in South America, the Mediterranean littoral, Eastern Europe, the Middle East, East Africa, Central Asia, China, Russia, and Australia. After infection the parasites encyst, usually in the liver or (less commonly) in the lungs. Although rare, cysts can grow ectopically in almost any organ in the body, with the kidneys being rare involvement [2]. Renal involvement is documented in 2–3% of total hydatid disease which is very less compared to liver and lung involvement [1]. Isolated renal hydatid disease is even rarer [3].
Initially, cysts are asymptomatic, but over time they enlarge (1–2 cm/yr) and eventually cause pain or a palpable abdominal mass; hydatiduria and renal colic occur in a minority of patients. Renal function is usually unaffected. Imaging shows a thick-walled, fluid-filled spheric cyst, often with a calcified wall; the appearance helps define the stage of the disease and, in turn, management strategies. Serologic testing is adjunctive for diagnosis, with a sensitivity of only 60% to 90%. Although use of percutaneous puncture, aspiration, injection, and reaspiration (PAIR) is a good therapeutic option for liver cysts, this is not done for lung or renal cysts, for which the only options are surgical resection or antiparasitic chemotherapy. Albendazole (400 mg orally twice per day for 1 to 6 months) is the recommended medical therapy [4]. Surgical excision is indicated in some patients because of the size or location of the lesions. Cyst rupture can cause anaphylaxis. Some evidence suggests that Praziquantel plus albendazole preoperatively and postoperatively may minimize secondary seeding and metastatic infection [5].
Acknowledgement
The authors acknowledge all the ward staff who took care of the patient.
Funding
None.
Availability of Data and Materials
The data supporting the conclusions of this article are available as an electronic medical record.
Author Contributions
Study concept and design: Dr, Vineet Ajitsaria, Dr Krupal Patel; Data acquisition: Dr Amit Agrawal, Dr Sahil Agrawal; Data analysis: Dr Vineet Ajitsaria, Dr Krupal Patel; Drafting of manuscript: Dr Krupal Patel; Critical revision of the manuscript: Dr Vineet Ajitsaria, Dr Sahil Agrawal, Dr Amit Agrawal.
Conflicts of Interest
None.
Consent
Informed written consent was obtained from the patient for publication of this manuscript and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Ethical Approval
Not applicable.
Article Info
Article Type
Case ReportPublication history
Received: Thu 19, May 2022Accepted: Mon 04, Jul 2022
Published: Wed 27, Jul 2022
Copyright
© 2023 Krupal Patel. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.AJSCR.2022.02.01
Figures & Tables
References
1.
Bhandarwar AH,
Tayade MB, Makki K, Mhaske S (2009) Primary Renal Hydatid Cyst. Bombay Hosp
J 51: 401-404.
2.
Campbell-Walsh-Wein
Urology, 12th Edition. ISBN: 978-0-323-54642-3.
3.
Kalinova K, Usunov
N (2007) Primary renal echinosossis—an experiment with 14 cases. J IMAB Ann
Proc (Scientific Papers) 13: 5-7. book 1.
4. Kappagoda S, Singh U, Blackburn BG (2011) Antiparasitic therapy. Mayo Clin Proc 86: 561-583. [Crossref]
5. Bygott JM, Chiodini PL (2009) Praziquantel: neglected drug? Ineffective treatment? Or therapeutic choice in cystic hydatid disease? Acta Trop 111: 95-101. [Crossref]