A Device for Polypectomy May Contribute to Safety in Bloodless Resection of a Small Hemangioma of the Tongue under Local Anesthesia
A B S T R A C T
Hemangiomas require appropriate treatments with controlled intraoperative bleeding. Even for a small hemangioma, the treatment is usually provided under general anesthesia to control bleeding. However, in the case of the patients who are at high risk of surgery under general anesthesia, a surgical treatment method must be considered under local anesthesia. We performed polypectomy for the resection of a small tongue hemangioma in an 88-year-old patient under local anesthesia. The device for polypectomy is suitable for the resection of a small hemangioma of the tongue, even for a patient who is at risk for surgery under general anesthesia.
Keywords
Polypectomy, hemangioma, tongue, bloodless
Introduction
Hemangiomas require appropriate treatments with controlled intra-operative bleeding, especially in the oral cavity [1]. It is difficult to control bleeding by conventional surgical methods because hemangioma is a benign tumor of dilated blood vessels. These treatments usually were performed under general anesthesia to control safety hemostasis. Polypectomy is underutilized for small polyp resection despite its favorable safety and efficacy [2]. A device of polypectomy made by Martin Co. Ltd. (Germany) automatically outputs small current for alternating incisions and coagulations for fast bloodless excision. This method is useful for resection of small polyps and pedicled polyps under local anesthesia.
Technical Note Report
Recently, we tried to use the device for polypectomy of a small tongue hemangioma in a patient. The patient was an 88-year-old woman with small hemangiomas on the lateral surface of the tongue (Figure 1). The size recorded was a 15x10mm solid tumor by ultrasound examination (Figure 2). The treatment under general anesthesia could not be performed due to her serious heart disease. Therefore, we had to set up a new safe treatment under local anesthesia. 2% Lidocain 2.6-mL without adrenalin was used to prevent the hemangioma from shrinkage (Figure 3). Three minutes after local anesthesia, the operation was started. At first, a ring of the device was fitted around the hemangioma. Secondly, the hemangioma was softly grasped with forceps and raised upward for excision. Then, the hemangioma was completely resected by the polypectomy device with slow secure hemostasis and cutting of the surrounding tongue muscle, including the invisible micro-veins (Figure 4). The time required for resection was around 15 seconds, and the amount of blood loss was extremely small, i.e., less than 1g. The wound was closed by 4/0 nylon surgical suture (Figure 5). There were no postoperative local complications, and wound healing was good. At 2-week postoperative follow-up, the symmetry of the tongue was confirmed (Figure 6). The histopathological report confirmed the diagnosis of cavernous hemangioma.
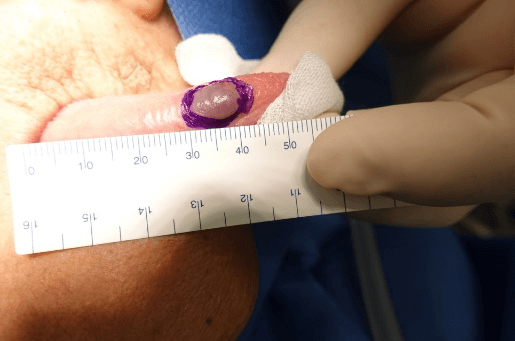
Figure 1: Isolated hemangioma on the right side of the tongue sixed 15x10cm.
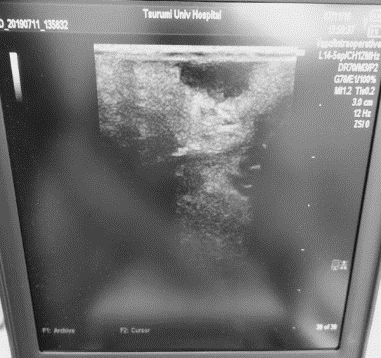
Figure 2: Ultrasonic examination of the solid hemangioma located on the right side of the tongue.
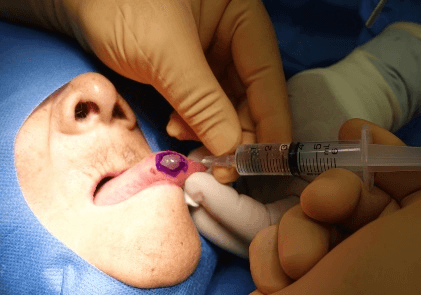
Figure 3: 2% Lidocain 2.6-mL without adrenalin was used to prevent the hemangioma from shrinkage.
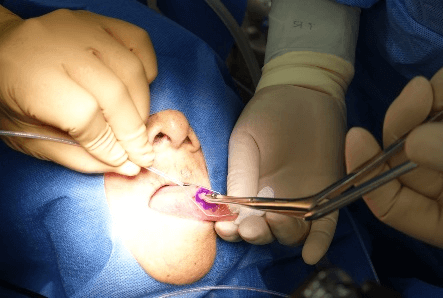
Figure 4: Excision the surface layer of the periphery of hemangioma by the polypectomy device.

Figure 5: The wound was closed by 4/0 nylon surgical suture.
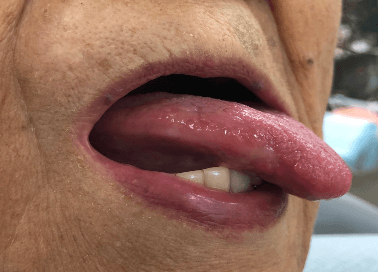
Figure 6: Finding at 2 weeks post operation.
Discussion
The appearance of cavernous hemangioma rarely occurs on the tongue. The early stage of hemangioma may be very cellular with solid nests of plump endothelial cells and little vascular lumen. The localized and superficial hemangiomas of the tongue were treated by conventional resection with cold knife, cauterization by Plasma Knife surgery with radiofrequency (PK), and intralesional laser treatment. It was difficult to control bleeding during surgical excision with cold knife. The tongue hemangioma requires careful consideration for consequent bleeding [1]. As a conservative treatment, intra lesional laser treatment of the tongue vascular lesions was effective; however, slight paresthesia and ulcer formation occurred as complications [3]. PK was developed as a new cautery. There was no bleeding during the cauterization of the small hemangioma and no recurrence postoperatively; however, the wound healing required around three weeks [4].
The resection using the device for polypectomy for the treatment of small tongue hemangioma was controlled under local anesthesia with some advantages, including the points of bloodless and short surgery, with less complications in comparison to the other treatments mentioned above. However, gastrointestinal bleeding is the most common serious adverse event with reported risks of 0.1–0.6% [5]. To prevent postoperative bleeding, just in this case, the wound was closed by 4/0 nylon suture.
In conclusion, the device for polypectomy is one of the feasible devices for resection of a small hemangioma of the tongue, even for a patient who is at risk for surgery under general anesthesia.
Conflicts of Interest
None.
Ethical Approval
Not applicable.
Consent
The patient has given permission to publish the paper.
Article Info
Article Type
Case ReportPublication history
Received: Thu 02, Apr 2020Accepted: Mon 20, Apr 2020
Published: Wed 22, Apr 2020
Copyright
© 2023 Koji Kawaguchi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JSO.2020.02.06
Figures & Tables
References
- Kripal K, Rajan S, Ropak B, Jayanti I (2013) Cavernous hemangioma of the tongue. Case Rep Dent 2013: 898692. [Crossref]
- Tate DJ, Desomer L, Heitman SJ, Forbes N, Burgess NG et al. (2020) Clinical implications of decision making in colorectal polypectomy: an international survey of Western endoscopists suggests priorities for change. Endosc Int Open 8: E445-455. [Crossref]
- Miyazaki H, Kato J, Watanabe H, Harada H, Kakizaki H et al. (2009) Intralesional laser treatment of voluminous vascular lesions in the oral cavity. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 107: 164-172. [Crossref]
- Kutluhan A, Bozdermir K, Ugras S (2008) The treatment of tongue haemangioma by plasma knife surgery. Singapore Med J 49: e312-e314. [Crossref]
- Ko CW, Dominitz JA (2010) Adverse events of colonoscopy: magnitude and management. Gastrointest Endosc Clin N Am 20: 659-671. [Crossref]