A Long-Term and Sustainable Response to Orapali in a BRCA2 Mutant Advanced Pancreatic Cancer: A Case Report
A B S T R A C T
Pancreatic cancer is a highly malignant cancer characterized by high mutation rates of oncogenes and tumor suppressor genes and genomic instability. It has a poor prognosis owing to early metastasis and rapid growth. Therefore, new drugs or treatments are urgent to be required. Poly ADP-Ribose polymerase (PARP) inhibitors have shown therapeutic efficacy in pancreatic cancer driven by defects in homologous recombinant (HRD). Here we report a case of advanced pancreatic cancer with BRCA2 mutation. The patient came to our hospital due to abnormal enlargement of the left supraclavicular lymph node. Further examination revealed pancreatic cancer with multiple retroperitoneal lymph nodes metastases and lung metastases. Pathological and immunohistochemical results of supraclavicular lymph node confirmed it was pancreatic cancer metastasis. Next generation sequencing (NGS) demonstrated that BRCA2 germline mutation. Subsequently, gemcitabine combined with cisplatin as first line therapy was commenced for the patient. The tumors were significant reduced after 6 cycles of treatment. Then, the patient was given orapali (PARP inhibitors) to maintain treatment. Surprisingly, the efficacy has lasted for about 20 months (from Dec 2021 to Aug 2023) and no signs of disease progression have been found. Our case shows that orapali provides a more efficient and low-toxic treatment for patient with BRCA2 mutation advanced pancreatic cancer, which is expected to change the treatment pattern of advanced pancreatic cancer.
Keywords
Pancreatic cancer, BRCA2 mutant, orapali, PARP inhibitors
Introduction
In the past years, some changes have been emerged in the treatment of pancreatic cancer which is connected with the development of targeted therapeutic agents [1]. Owing to its hidden location, early metastasis and rapid growth, more than 80% of pancreatic cancer patients are in the advanced stage when they are diagnosed, result to poor prognosis and short median survival [2-3]. Currently, chemotherapy is still the first-line standard treatment for advanced pancreatic cancer. However, the efficacy is limited and prone to drug resistance.
The PARP inhibitor opens a new chapter in the precise treatment of advanced pancreatic cancer with BRCA1/2 mutation [4]. In recent years, PARP inhibitors have become the most commonly molecular targeted drugs for strain BRCA1/2 mutation. These drugs can retain normal cells while inducing cancer cell death [5]. These studies show that the PARP inhibitor may be effective and can bring clinical benefits to patients. In our case, we reported that a long-term and sustainable response to orapali in a BRCA2 mutant advanced pancreatic cancer.
Case Report
A 45-year-young woman was referred to our hospital for abnormal enlargement of the left supraclavicular lymph node. Abdominal and chest computed tomography (CT) showed that pancreatic cancer with multiple retroperitoneal lymph node, left supraclavicular lymph node and lung metastases. The maximum diameter of the tumor was about 10 cm (Figure 1A). Left supraclavicular lymph node biopsy was performed. Pathological and immunohistochemical results: CK7(+), CK19(+), CA19-9(+), CEA(-), CK8/18(+), CDX2(-), Ki67(+50%), PMS2(+), MLH1(+), MSH2(+), MSH6(+), CK20(-), Muc-1(+), Muc-2(-), Muc-5AC(-), GCDFP-15(-), GATA3(-), NapsinA(-), TTF-1(-), SYN(-), CgA(-), CD56(-). She was diagnosed with pancreatic cancer in Aug 2021. Next generation sequencing was also applied. Interestingly, the results showed that BRCA2 gene germline mutation.
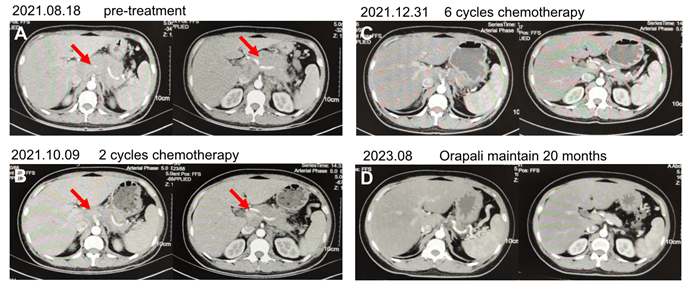
Figure 1: The image of abdominal computed tomography (CT).
A) Pre-treatment CT scan. Arrows indicate tumors. B) CT scan after two cycles of gemcitabine combined with cisplatin chemotherapy. Arrows indicate tumors. C) CT scan after six cycles of gemcitabine combined with cisplatin chemotherapy. D) CT scan after orapali has taken 20 months.
Subsequently, the patient was diagnosed advanced pancreatic cancer with BRCA2 mutation. We treated the patient with gemcitabine combined with cisplatin as first line therapy due to BRCA2 mutation in Aug 2021. After 2 cycles of treatment, as shown in (Figure 1B), the size of the tumor was significantly decreased compared with pre-treatment, resulting in a partial response. So the patient was performed 6 cycles chemotherapy (Figure 1C). Next, the patient was given PARP inhibitors (orapali, 300mg bid po) to maintain treatment.
Surprisingly, to date, orapali treatment for the patient had been continued about 20 months (from Dec 2021 to Aug 2023). As shown in (Figure 1D), no tumor was observed in the abdominal computed tomography. The patient achieved clinical complete remission of disease. She has not obvious clinical symptoms and no severe adverse events. She obtained a long-term survival because of orapali sustainable response. In summary, the patient was clinically diagnosed with BRCA2 mutant advanced pancreatic cancer and have a long-term and sustainable response to orapali (Figure 2).
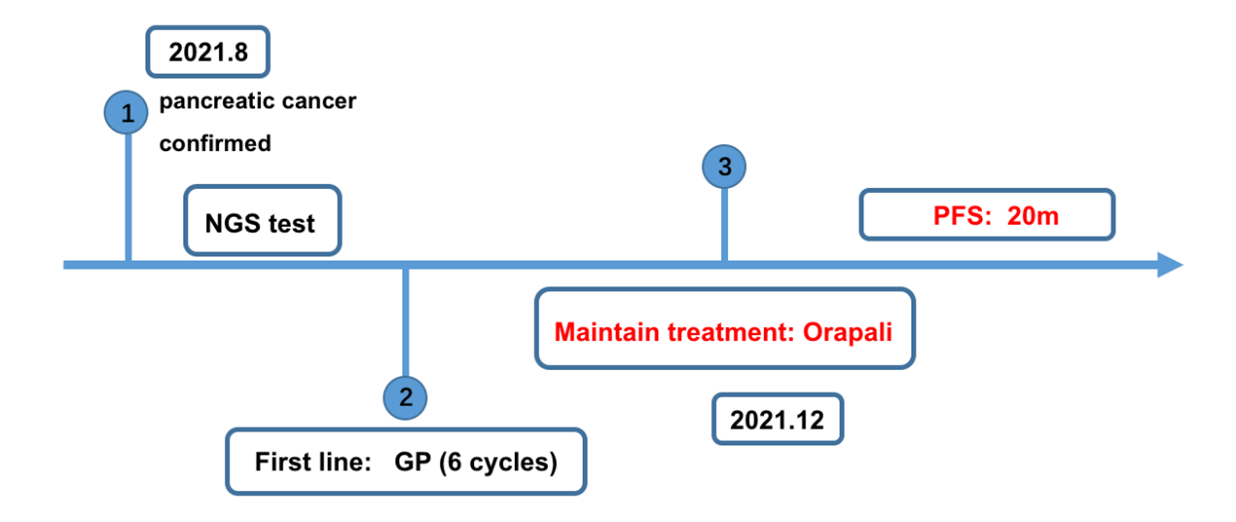
Figure 2: Treatment flowchart.
NGS: next generation sequencing. GP: gemcitabine combined with cisplatin chemotherapy.
Discussion
In our case, we described an advanced pancreatic cancer patient with a large tumor and BRCA2 mutant, who obtained a long-term and sustainable response to orapali. To our knowledge, the survival outcome of advanced pancreatic cancer patients was significantly worse. For BRCA2 mutant advanced pancreatic cancer patients, PARP inhibitors may be effective.
POLO study is the first randomized double-blind phase III clinical study to evaluate the efficacy of the PARP inhibitor (orapali) as a maintenance treatment after the first-line platinum containing chemotherapy for advanced pancreatic cancer with BRCA germline mutation. The results confirmed that progression free survival (PFS) was significantly prolonged in the orapali maintenance group compared to the placebo group, with a median PFS of 7.4 months vs 3.8 months, respectively (HR=0.53, 95% CI 0.35-0.82, P=0.004) [6]. Therefore, NCCN guidelines recommend that orapali can be used as a maintenance treatment for BRCA germline mutation advanced pancreatic cancer patients. In our case, the patient obtained 24 months PFS and to date, there was no indication for disease progression.
Recently, journal of clinical oncology published the final result of over survival (OS) data. The final OS results showed that the median OS of the two groups was similar, 19.0 months and 19.2 months, respectively, with no significant statistical difference between the two groups (HR=0.83, 95% CI 0.56-1.22, P=0.3487) [7]. Although OS data does not show statistical differences between orapali and placebo, PFS and other secondary endpoints support the maintenance of orapali in patients with embryonic BRCA mutations metastatic pancreatic cancer. In our case, we believe that BRCA2 mutation might be caused the protein of PARP increase. Therefore, such a good response is mainly due to the PARP inhibitor (orapali).
Taken together, we reported that a BRCA2 germline mutation metastatic pancreatic cancer patient, who has a long-term and sustainable response to orapali. In term of BRCA2 germline mutation metastatic pancreatic cancer, PARP inhibitor may be an effective therapeutic option.
Acknowledgements
The authors would like to thank the patient for the publication of clinical data and images.
Conflicts of Interest
None.
Article Info
Article Type
Case ReportPublication history
Received: Tue 15, Aug 2023Accepted: Wed 30, Aug 2023
Published: Thu 07, Sep 2023
Copyright
© 2023 Xiuming Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2023.05.03
Figures & Tables
A) Pre-treatment CT scan. Arrows indicate tumors. B) CT scan after two cycles of gemcitabine combined with cisplatin chemotherapy. Arrows indicate tumors. C) CT scan after six cycles of gemcitabine combined with cisplatin chemotherapy. D) CT scan after orapali has taken 20 months.
NGS: next generation sequencing. GP: gemcitabine combined with cisplatin chemotherapy.
References
1. Park W, Chawla A,
O'Reilly EM (2021) Pancreatic Cancer: A Review. JAMA 326: 851-862. [Crossref]
2. Siegel RL, Miller
KD, Fuchs HE, Jemal A (2021) Cancer statistics, 2021. CA Cancer J Clin
71: 7-33. [Crossref]
3. Rawla P, Sunkara T,
Gaduputi V (2019) Epidemiology of pancreatic cancer: global trends, etiology
and risk factors. World J Oncol 10: 10-27. [Crossref]
4. Waddell N, Pajic M,
Patch AM, Chang DK, Kassahn KS et al. (2015) Whole genomes redefine the
mutational landscape of pancreatic cancer. Nature 518: 495-501. [Crossref]
5. Aguirre AJ, Nowak
JA, Camarda ND, Moffitt RA, Ghazani AA et al. (2018) Real-time genomic
characterization of advanced pancreatic cancer to enable precision medicine. Cancer
Discov 8: 1096-1111. [Crossref]
6. Golan T, Hammel P, Reni M, Cutsem EV, Macarulla T et al. (2019) Maintenance olaparib for germline BRCA-mutated metastatic pancreatic cancer. N Engl J Med 381: 317-327. [Crossref]
7. O’Reilly EM, Lee JW, Zalupski M, Capanu M, Park J et al. (2020) Randomized, multicenter, phase ii trial of gemcitabine and cisplatin with or without veliparib in patients with pancreas adenocarcinoma and a germline BRCA/PALB2 mutation. J Clin Oncol 38: 1378-1388. [Crossref]