An Intramuscular Epidermal Cyst of Erector Spinae Muscles: A Case Report
A B S T R A C T
An intramuscular epidermal cyst without subcutaneous involvement is extremely rare. The patient presented with low back pain. Spinal magnetic resonance imaging indicated spindle-shaped mass in the right erector spinae muscles located at L3 to L5 level without any connection with subcutaneous tissue. The patient underwent operation for removal of intramuscular cystic lesion. The tumor was totally removed and pathologically confirmed with epidermal cyst. Unlike typical epidermal cyst, the patient had a characteristic clinical manifestation of mild low back pain without palpable mass and local tenderness.
Keywords
Intramuscular epidermal cyst, cystic mass, muscle pain
Introduction
An epidermal cyst commonly occurs in subcutaneous tissues. It typically involves hair-bearing tumor at the various body parts [1, 2]. It is usually benign, composed of true epidermis confined by a wall of stratified squamous epithelial cells and mostly detected by palpable mass. Sternomastoid, presacral, intraosseous, and splenic epidermal cysts were reported as the unusual sites of epidermal cysts [3-5]. However, an intramuscular epidermal cyst without subcutaneous tissue involvement is extremely rare. In the present report, we describe diagnostic image findings and management of the epidermal cyst confined to the muscle layer without subcutaneous involvement.
Case Report
A 49-year-old woman was admitted to our hospital with a complaint of worsening lower back pain for five years. She had been treated with only analgesic medications at other hospitals under a diagnosis of lumbar sprain without radiologic evaluation, such as lumbar magnetic resonance imaging (MRI) or lumbar computed tomography (CT). The numeral rating scale was 3 at the admission of hospital. Physical examinations indicated that there was only mild tenderness at the right side paraspinal muscle of lower lumbar level without palpable mass or color change of the skin. She had no previous history of trauma or surgery at the area. Simple lumbar radiograph didn’t show any abnormal finding. CT presented homogenous hypodensity lesion without hemorrhage or calcification in right erector spinae muscles located at L3 to L5 level (Figure 1C), whereas MRI demonstrated a large well-defined and spindle-shaped mass lesion with minimal enhancement measuring 2.8cm x 7.5cm x 4.1cm. The lesion was isointense on T1-weighted images and hyperintense on T2-weighted images, and it located totally within the erector spinae muscles without subcutaneous involvement (Figures 1A, 1B, 1D, 1E). Preoperative differential diagnosis included intramuscular lipoma, chronic hematoma, ganglion cyst, and granuloma.
The lesion was removed through a vertical skin incision in the L3-5 level. According to surgical findings, the mass was yellow-pinkish, and its boundary was clearly distinguished. Muscle tissue completely enveloped the mass without any defect in the fascia or muscle layer over it. It was completely removed. Her low back pain disappeared after the surgery. Gross findings showed that the mass contained sebaceous material with cystic components without definitive hair structure. According to a histopathological examination, the mass was diagnosed as epidermal cyst with keratinizing stratified squamous epithelium and hair follicle (Figure 2).

Figure 1: An intramuscular epidermal cyst without subcutaneous tissue involvement at L3 to L5 level in the right erector spinae muscles. A) & B) In sagittal and axial T2-weighted magnetic resonance imaging (MRI) reveal hyperintense cystic mass (white arrow) without involvement to the subcutaneous level. C) Computed tomography shows homogenous low-density mass lesion (white arrow). D) Sagittal T1-weighted MRI shows well-defined lesion (white arrow) with homogenous low signal intensity. E) Gadolinium-enhanced T1-weighted image reveals rim enhancement (white arrow) of cyst wall.
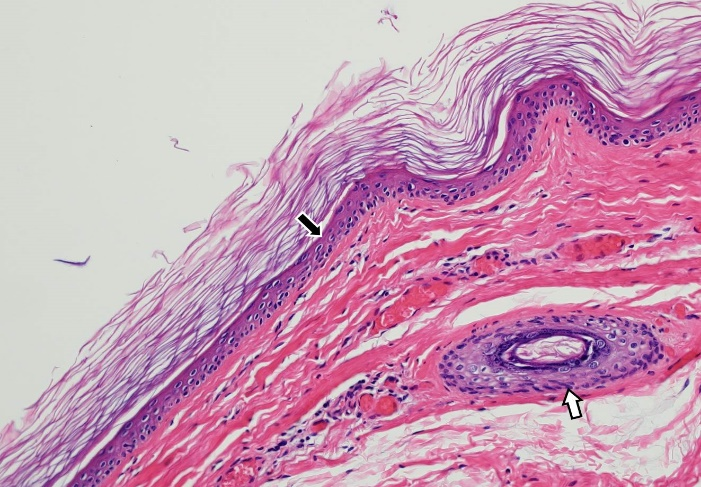
Figure 2: Pathological findings show composition of keratinizing stratified squamous epithelium (black arrow) and hair follicle (white arrow) (Hematoxylin and eosin stain, x100).
Discussion
The subcutaneous epidermal cyst is a lesion commonly encountered by surgeons, and its incidence rate is known about 85-90% of subcutaneous cysts [6]. It would be found at any age, while it is more frequent between 3 and 4 decades [7]. The causes of proliferation of the epidermal cyst are unclear, but genetic factors such as Gardner syndrome and Gorlin syndrome have been suggested having relationship with it [8]. In patient with Gardner syndrome, epidermal cysts may be occurred on atypical area and this disease can associated with colorectal polyps [9]. The other mechanism is that traumatic or surgical history cause the epidermal cyst [10]. We didn’t perform genetic study in this case, but there was no predisposing factor such as trauma or surgery.
Most epidermal cysts are benign and confined to the skin or subcutaneous level. The scalp, face, neck, and trunk are commonly involved sites. But any area of body such as buttock, palmoplantar, genitalia, and nipple could be involved [11]. The lesions could be solitary or multiple. Generally, physical examination may reveal a firm, palpable, and painless mass. Although it is usually an asymptomatic lesion, some cases with inflammatory changes including erythema, swelling, tenderness, and even stench caused by cyst rupture have been reported [12]. Our patient complained only lower back pain, which was unusual presentation in the reported cases of epidermoid cysts. Her lower back pain improved after tumor removal. In addition, the patient didn’t show palpable mass or local tenderness. All of these findings seem to be characteristic clinical features of the intramuscular epidermoid cyst.
The radiological evaluations with CT and MRI are necessary to diagnose the epidermal cyst and set a surgical strategy. CT findings are known to show well-confined low-density cystic lesions due to fat and keratin with wall enhancement on contrast-enhanced CT [13]. On MRI, typical epidermoid cysts demonstrate hypo or isointense signals on T1-weighted images and hyperintense on T2-weighted images with rim enhancement of the cystic wall, which can be changed by cystic components of keratin and fat [13, 14].
The CT and MRI findings of the mass itself in our patient were quite similar to those of previous reports. However, in the present case, the epidermal cyst was confined to the erector spinal muscle without subcutaneous involvement. The MRI demonstrated low-signal intensity on T1-weighted image and high signal intensity on T2-weighted image without septation and mildly enhanced on cyst margin. To our knowledge, the intramuscular epidermal cyst without subcutaneous tissue involvement was only one case in the literature [4].
There are some reports about intramuscular epidermal cysts. One of them is similar to our case, which was about an epidermal cyst located in the sternomastoid muscle of the neck without subcutaneous tissue involvement [4]. However, it seems to be different from our case because it may have been caused by trauma. In another report, an epidermal cyst occurred in the gluteus maximus muscle, which was different from ours in that the cyst extended from the subcutaneous level due to the cystic rupture [15]. As far as we know, this is the first case that epidermal cyst confined to lumbar paravertebral muscle.
Conclusion
The epidermal cyst confined to muscle layer without subcutaneous tissue involvement is known to be very rare. In the present case, the image findings were characteristic as previous reports, but the patient showed an unusual clinical presentation, only lower back pain without palpable mass or skin discoloration. The intramuscular epidermoid cyst in lumbar area seems to be indicated for surgery because it can cause lower back pain.
Conflicts of Interest
None.
Article Info
Article Type
Case ReportPublication history
Received: Mon 16, Mar 2020Accepted: Mon 06, Apr 2020
Published: Wed 08, Apr 2020
Copyright
© 2023 Seung Won Park . This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.03.09
Figures & Tables
References
- Hoang VT, Trinh CT, Nguyen CH, Chansomphou V, Chansomphou V et al. (2019) Overview of epidermoid cyst. Eur J Radiol Open 6: 291-301. [Crossref]
- Yang DM, Yoon MH, Kim HS, Oh YH, Ha SY et al. (2001) Presacral epidermoid cyst: imaging findings with histopathologic correlation. Abdom Imaging 26: 79-82. [Crossref]
- Garg M, Kataria SP, Sethi D, Mathur SK (2013) Epidermoid cyst of spleen mimicking splenic lymphangioma. Adv Biomed Res 2: 49. [Crossref]
- Chatterjee P, Chandra A, Dastidar N (1976) Epidermal cyst in sternomastoid muscle simulating a malignant growth. Indian J Otolaryngol 28: 86-87.
- Patel K, Bhuiya T, Chen S, Kenan S, Kahn L (2006) Epidermal inclusion cyst of phalanx: a case report and review of the literature. Skeletal Radiol 35: 861-863. [Crossref]
- Lever WH, Lever GS (1997) Tumors and cysts of epidermis. In Elder D, eds. Histopathology of the Skin, 8th ed. Lippincott-Raven, Philadelphia: 685-746.
- Zito PM, Scharf R (2019) Cyst, Epidermoid (Sebaceous Cyst). StatPearls [Internet] 2020. [Crossref]
- Balasundaram P, Garg A, Prabhakar A, Joseph Devarajan LS, Gaikwad SB et al. (2019) Evolution of epidermoid cyst into dermoid cyst: Embryological explanation and radiological-pathological correlation. Neuroradiol J 32: 92-97. [Crossref]
- Dutta M, Saha J, Biswas G, Chattopadhyay S, Sen I et al. (2013) Epidermoid cysts in head and neck: our experiences, with review of literature. Indian J Otolaryngol Head Neck Surg 65: 14-21. [Crossref]
- Glusac EJ (1999) Lever's Histopathology of the Skin, Eighth Edition. Lippincott Williams & Wilkins, Baltimore: 237.
- Low SF, Sridharan R, Ngiu CS (2015) Giant epidermal cyst with intramuscular extension: a rare occurrence. BMJ Case Rep 2015: bcr2013202534. [Crossref]
- Wollina U, Langner D, Tchernev G, Franca K, Lotti T (2018) Epidermoid Cysts - A Wide Spectrum of Clinical Presentation and Successful Treatment by Surgery: A Retrospective 10-Year Analysis and Literature Review. Maced J Med Sci 6: 28-30. [Crossref]
- Bin Manie MA, Al Qahtani KH, Al Ammar A, Islam T, Otaibi FNA (2020) Epidermoid cyst of the suprasternal region: a rare case report. Braz J Otorhinolaryngol 86: 133-135. [Crossref]
- Pires Goncalves L, Silva C, Teixeira M, Costa Dias S, Sousa Mendes V (2011) Testicular epidermoid cyst - Ultrasound and MR typical findings with macroscopy correlation. Int Braz J Urol 37: 534-535. [Crossref]
- Yim YH, Kim NR, Moon SG (2018) Intramuscular Epidermal Cyst of the Buttock: A Case Report. Journal of the Korean Society of Radiology 79: 354-358.