Journals
Calcified constrictive pericarditis treated with ultrasonic devices
A B S T R A C T
A 52-year-old male patient was diagnosed as constrictive pericarditis with severe diastolic dysfunction, which was characterized by broadly calcified pericardium on fragile parts of the heart: the right atrium, both coronary vessels as well as the right and left ventricles. We successfully conducted a total pericardiectomy with an ultrasonic aspirator to break the calcified pericardium into smaller parts and an ultrasound scalpel to peel off the debris.
K E Y W O R D S
Constrictive, pericarditis, calcification, heart, failure, ultrasonic surgery
Abbreviation
CP: constrictive pericarditis , LV: left ventricle, RV: right ventricle
Introduction
Constrictive pericarditis (CP) is an uncommon chronic inflammatory condition characterized by pericardial fibrosis and occasional calcification that limits diastolic ventricular filling. In cases where medical treatment is not effective, surgical intervention is demanded [1].
Radical pericardial resection is desirable but technically difficult because of the risks of myocardial injury especially with broadly calcified pericardium. As an alternative technique, pericardiotomy known as the “waffle procedure” has been proposed [2]. However, for patients with heavy calcification, this technique is not possible.
We present a case of broadly calcified CP with severe diastolic dysfunction in which a combination of ultrasonic scalpel and aspirator could successfully remove diffuse calcification without massive bleeding or hemodynamically disturbing cardiac arrhythmia.
Case Report
A 52-year-old male presented to the emergency department with dizziness and shortness of breath. He also described increased abdominal circumference, lower extremity edema bilaterally and 20 kg weight gain in past few months. His past medical history was unremarkable except for type 2 diabetes mellitus.
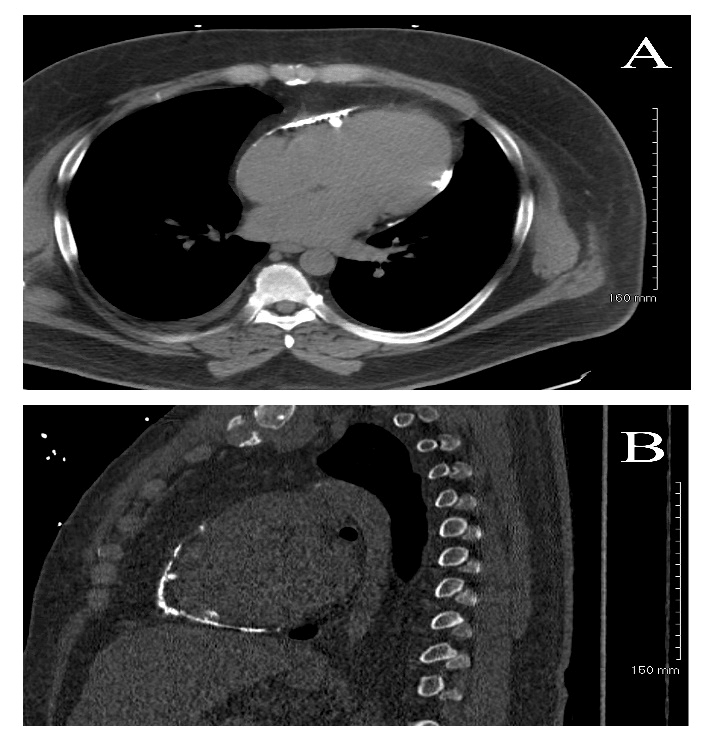
A chest radiograph revealed a high-density line surrounding the heart (Figure 1). Transthoracic echocardiogram revealed severe diastolic dysfunction consistent with constrictive pericarditis; LV ejection fraction was 40 %, functional shortening was 11 %, mitral valve E/A ratio was 2.2, lateral E’ was 3.0 cm/s, lateral E/E’ was 18.8 and deceleration time was 130 msec. RV pressure was 40 mmHg and estimated central venous pressure was 20 mmHg. Diastolic septal bounce was noted, and the pericardium appeared broadly thickened to 4 mm. Computed tomography discovered pericardial calcification which covered the majority of the surfaces the right atrium and of both ventricles (Figure 2).
A cardiac catheterization showed severely elevated and equalization of diastolic pressures in both ventricles and “square-root” signs; LV end diastolic pressure was 22 mmHg, RV end diastolic pressure was 22 mmHg, right atrial pressure was 21 mmHg, and pulmonary wedge pressure was 22 mmHg.
Laboratory studies including hepatitis panel, ferritin, and Interferon-gamma release assays for tuberculosis infection were all negative. The etiology was idiopathic in this patient. The diagnosis of chronic constrictive pericarditis was established, and surgical intervention was undertaken.

Procedure and Outcomes
A median sternotomy was performed. There were dense adhesions in the mediastinal and pericardial spaces, but most surfaces of the great vessels and heart except the posterior and inferior wall of LV were exposed without incident by an ultrasound scalpel (Harmonic scalpel, Ethicon US, Cincinnati, USA).
There was a large calcified pericardium (10 x 10 cm) on the right atrium, RV free wall and LV anterior wall. Here we decided to use an ultrasound aspirator (SONOPET, Stryker, Kalamazoo, USA) to divide the large calcified plaque into small pieces. Then these pieces were removed from the epicardium by Harmonic scalpel.
Next, the LV apex was lifted with a stabilizer to expose the calcified and thickened posterior and inferior pericardium of LV, which was removed in the same fashion. Using this new method, the surface of the heart was safely released from the thick and calcified pericardium. The cardiac retraction was well tolerated hemodynamically; therefore, cardiopulmonary bypass was not used in this patient. The patient was extubated on the day of surgery and discharged on postoperative day 5. Post-operative trans-esophageal echocardiogram revealed improved cardiac function; LV ejection fraction was 55 %, E/A ratio was 2.0, lateral E’ was 10.3 cm/s and lateral E/E’ was 6.2.
Discussion
Chronic constrictive pericarditis is relatively unusual, and severely calcified constrictive pericarditis is exceptionally rare. Some case reports are published however, the appropriate surgical management has not been well established [3, 4].
Overall early mortality rate after pericardiectomy is reported to be 2.5 % nowadays [1]. The waffle procedure, ultrasonic scalpel, aspirator, and off-pump procedure contribute to reduce the risk of this surgery [2, 3, 5]. However, among surgical complications, bleeding from the epicardium and muscle is still one of the major concerns.
This patient had a calcified cage around the fragile tissue such as the right atrium and coronary vessels, so we considered this patient had extraordinarily high risk for hazardous injury. Rough maneuvers should be avoided, but on the other hand, it was time consuming to remove the large calcium with a single fine ultrasonic aspirator. Therefore, we used the SONOPET to break the plaque into small parts, and the small debris was removed by Harmonic scalpel.
Funding statement and Conflict of interest statement
None.
Article Info
Article Type
Case ReportArticle History
Received: 5 October, 2018Accepted: 25 October, 2018
Published: 14 October 2018
Copyright
© 2018 Kosuke Ujihira. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.10.31487/j.SCR.2018.03.012
Author Info
Corresponding author
Kosuke UjihiraDivision of Cardio-thoracic surgery, Department of Surgery, University of Wisconsin School of Medicine and Public Health, 600 High Land Avenue, Madison, WI 53792, USA;
Figures & Tables
References
- Gillaspie EA, Stulak JM, Daly RC, Greason KL, Joyce LD, et al. (2016) A 20-year experience with isolated pericardiectomy: Analysis of indications and outcomes. J Thorac Cardiovasc Surg 152: 448-458. [Crossref]
- Heimbecker RO, Smith D, Shimizu S, Kestle J (1983) Surgical technique for the management of constrictive epicarditis complicating constrictive pericarditis (the waffle procedure). Ann Thorac Surg 36: 605-606. [Crossref]
- Gallo I, Saenz A, Alonso C, Cesari F, Larman M, et al. (1991) Calcified constrictive pericarditis. Ultrasonic debridement. Eur J Cardiothorac Surg 5: 391-392 [Crossref]
- Sanhueza ME, Torres R, Segura P, Villalobos A, Segovia E (2016) The Fortress Becomes a Prison: Calcified Constrictive Pericarditis. Am J Med 129: 263-265. [Crossref]
- Matsuura K, Mogi K, Takahara Y (2015) Off-pump waffle procedure using an ultrasonic scalpel for constrictive pericarditis. Eur J Cardiothorac Surg 47: e220-222. [Crossref]