Cross-Sectional, Non-Randomized, Single-Blinded, and Single-Center Study for the Accuracy of 12 Lead Smartphone ECG in the Detection of Ventricular Arrhythmias
A B S T R A C T
Since ventricular arrhythmias are frequently transitory, diagnosing them can be difficult. It has been investigated in the past to diagnose atrial fibrillation (AF) using a smartphone-based ECG. Data on the diagnostic efficacy of smartphone-based ECGs for ventricular arrhythmias, however, is insufficient.
Objective: Objectives of this study were a) to evaluate the accuracy of the spandan 12 lead ECG device in detection of the ventricular arrhythmias in comparison to the cardiologist, b) to evaluate the arrhythmia detection accuracy of the conventional ECG machine and spandan smartphone ECG machine to cardiologist diagnosis, and c) to detect spontaneous ventricular arrhythmias (VAs), namely ventricular tachycardia (VT) and supraventricular ectopic (SVE), ventricular ectopics (VE), ventricular premature complexes (VPCs), AV-block and ventricular ectopics (VE) can be fatal. Patients who are susceptible to VT/SVTs always have a risk of sudden cardiac death.
Methods: This cross-sectional study, single blinded and single-centric study was carried out at Shri Mahant Indresh Hospital (SMIH), Dehradun from 02-Aug-2022 to 29-Dec-2022. Patients with (n=1137) chest pain, syncope, palpitation, shortness of breath were enrolled from ECG department. A final total of 84 participants considered for the accuracy of interpretation of ventricular arrhythmia detected by the gold standard 12 lead ECG and smartphone-based ECG device along with the cardiologist’s diagnosis.
Results: Mean age (SD) was 54.42±14.58 years. The male gender (65.89%) shows the maximum frequency than female gender. Confusion matrix was referred to derive true positive cases for 12 lead standard ECG and smartphone ECG along with the cardiologist’s diagnosis was 46 as compared to 30 from 12 lead gold standard. Sensitivity of smartphone spandan ECG (35.38%) was better than gold standard 12 lead ECG (15.625%), and, PPV and NPV of smartphone spandan ECG was recorded to be better than gold standard 12 lead ECG. Ventricular arrhythmia was detected correctly in 46 (54.7%) cases and 30 (36.58%) cases by smartphone ECG and 12 lead gold standard, respectively.
Conclusion: Mobile ECG based devices can be used for detecting the arrhythmias as its overall accuracy of smartphone ECG in detecting the arrhythmias increase by 66.8%, i.e. the significance rise in accuracy of computer interpretation when compared to the cardiologist’s diagnosis.
Keywords
Accuracy, smartphone, specificity, sensitivity, validation, ventricular arrhythmias
Introduction
A somewhat prevalent kind of cardiovascular illness is ventricular arrhythmias. Arrhythmias are often seen in the majority of cardiovascular disorders [1]. Several different arrhythmias might manifest as symptoms. In many clinical situations, some, like premature ventricular and atrial contractions, may be benign [2]. Some of these conditions, such third-degree heart block and ventricular tachycardia, can be fatal. Others, like atrial fibrillation, are more problematic. The frequency of arrhythmia symptoms and the severity of their debilitating effects might vary [3]. The patient's symptoms, family history, and first ECG results might indicate an underlying rhythm that is more or less problematic [4].
An electrocardiogram (ECG) is frequently used in clinical practice to identify and can be utilised as a main diagnostic tool for cardiovascular diseases. Ambulatory electrocardiography (ECG) enables prolonged arrhythmia monitoring in a practical context [5]. To assist practitioners in understanding the various ambulatory ECG devices available and how to utilise them in clinical practice, a number of recommendations have been published. The most recent classification, done in 2017 by the international society for holter and non-invasive electrocardiology and heart rhythm society, ambulatory cardiac monitoring indications are separated into three main groups: diagnosis, prognosis, and arrhythmia evaluation [6-9].
Smartphone technologies are now pervasive and easily accessible in both affluent and developing countries, making them almost universal in their existence and penetration globally. Sunfox Technologies Private Limited's new spandan smartphone ECG gadget makes the claim that it can identify seven different forms of ventricular arrhythmias. After this technology has been clinically shown to deliver reliable and accurate diagnosis, non-medical persons may be able to utilise it anywhere in the globe. This technology may make it possible for even skilled medical staff in resource-constrained nations like India, where standard ECG equipment are not often accessible, to obtain a solid 12-lead ECG trace at a low cost [10-14].
The aims of this study were a) to evaluate the accuracy of the spandan 12 lead ECG device in detection of the ventricular arrhythmias in comparison to the cardiologist, b) to evaluate the arrhythmia detection accuracy of conventional ECG machine and spadnan smartphone ECG machine to cardiologist diagnosis, and c) to detect spontaneous ventricular arrhythmias (VAs), namely ventricular tachycardia (VT) and supraventricular ectopics (SVE), ventricular ectopics (VE), ventricular premature complexes (VPCs), AV-block and ventricular ectopics (VE) can be fatal. Patients who are susceptible to VT/SVTs always have a risk of sudden cardiac death.
Methodology
Participants in the study were those who entered the ECG room at Shri Mahant Indiresh Hospital (SMIH), Dehradun, Uttarakhand, India, between 02-Aug-2022 and 29-Dec-2022 with a prescription for an ECG screening. Upon obtaining their written informed consent, we conducted this cross-sectional study at a single center that was not randomized, single-blinded, or multi-center. There were 1337 individuals in the final study population, who might be either male or female. By obtaining their written agreement and outlining the study's objectives, patients were included in the trial. The study eliminated patients with loose skin, ECGs recorded with electrical anomalies, or who were unable to give informed permission. Patients with chest pain, syncope, shortness of breath, or palpitations were included in the study.
I Analysis of Ventricular Arrhythmias
Ventricular tachycardia, AV-block, high degree AV-block, supraventricular ectopic, ventricular ectopic, supraventricular tachycardia, and V-paced rhythm were the ventricular arrhythmias that were taken into consideration for this study. According to guidelines offered by Sunfox Technologies Private Limited, ECGs were created and viewed. When the ECGs were collected, the patients were lying down and relaxed. After receiving clearance to do so, the patients followed the research nurses' directions and lay down. The 12-lead recording and the digital data were sent to a Google cloud-based server for subsequent analysis with the help of a spanish smartphone ECG-based application.
II 12-Lead ECG Acquisition
Under the direction of a cardiologist, the BPL cardiart 9108 device was used to record the 12-lead ECGs using the spandan 12-lead ECG and the goldberg 12-lead ECG for 10 seconds each. Using a standard 12 lead ECG and a spandan 12 lead ECG, the nurse took participants' 10-second resting ECGs. A micro USB cable was used to link the device to an ECG recording program. A cloud-based server was then accessed to receive the ECG recording data. All 12-lead ECGs from a regular ECG machine and a smartphone 12-lead ECG machine were independently reviewed by a blinded committee of cardiologists for the diagnosis of ventricular arrhythmia. ECGs were categorized as true positive or false negative depending on whether the detection was accurate or incorrect.
III Statistical Methods
The data was composed on a spread sheet and vivid statistical analysis was completed. Assessment of the accuracy of arrhythmia detection was done by calculation of error in detection of ventricular arrhythmia as compared to cardiologist’s diagnosis.
Results
In total, 1137 patients with chest pain, syncope, palpitation, and shortness of breath were enrolled in the ECG department. A final total of 84 participants was considered for the accuracy of interpretation of ventricular arrhythmia detected on spandan, a smartphone-based ECG, and standard 12 lead ECG along with the comparison of the cardiologist’s diagnosis.
Below (Table 1) summarizes the baseline characteristics of the study population. The mean age was 54.42±14.58 years (range of years: 25 and above) and 881 patients (65.89%) were males and 455 subjects (34.03%) were females.
Table 2 summarizes the confusion matrix of ventricular arrhythmia detection for 12 lead standard ECG and smartphone ECG in comparison to cardiologist diagnosis for overall Evaluation. True Positive cases derived from confusion matrix for 12 lead standard ECG and smartphone ECG in comparison to cardiologist diagnosis was 46 as compared to 30 from 12 lead gold standard.
Table 1: Baseline characteristics of
the study population.
|
Parameters |
Overall patients (n=1337) |
Standard 12 Lead ECG |
12 Lead Smartphone ECG |
Cardiologist’s Diagnosis |
|
Age in years (Mean±SD)
years |
54.42±14.58 |
|||
|
Female, n(%) |
455 (34.03) |
|||
|
Male, n(%) |
881 (65.89) |
|||
|
BMI(Mean)(Kg/m2) |
24.34 |
|||
|
Chest pain |
239 |
|||
|
Palpitations |
49 |
|||
|
Shortness of breath |
94 |
|||
|
Hypertension |
87 |
|||
|
COVID-19 |
65 |
|||
|
Pacemaker implantation |
37 |
|||
|
Smoker |
141 |
|||
|
Diabetic |
204 |
|||
|
Subjects on
Anti-Coagulant Drugs |
500 |
|||
|
Subjects on Diuretics
Drugs |
234 |
|||
|
Subjects on Antacid |
293 |
|||
|
Subjects on
Anti-Hypertensive Drugs |
453 |
|||
|
Subjects on
Anti-Anginal Drugs |
123 |
|||
|
Anti-Hyperlipidemic
Drugs |
350 |
|||
|
Hyperglycimic Drugs |
75 |
|||
|
Arrhythmic ECG |
NA |
141 |
130 |
108 |
|
Non Arrhythmic ECG |
NA |
1196 |
1207 |
1229 |
Table 2: Confusion matrix of
ventricular arrhythmia detection for 12 lead standard ECG and smartphone ECG in
comparison to cardiologist diagnosis for overall evaluation.
|
Parameters |
12 lead Gold standard |
Smartphone ECG |
|
True Positive |
30 |
46 |
|
True Negative |
1113 |
1169 |
|
False Positive |
32 |
38 |
|
False Negative |
162 |
84 |
Table 3 summarizes the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of the standard ECG and 12 lead smartphone ECG for ventricular arrhythmia interpretation in comparison to cardiologist diagnosis. The sensitivity of smartphone spandan ECG (35.38%) was better than gold standard 12 lead ECG (15.625%), and the PPV and NPV of smartphone spandan ECG were recorded to be better than gold standard 12 lead ECG.
Table 3: The sensitivity,
specificity, positive predictive value (PPV), and negative predictive value
(NPV) of the standard ECG and 12 lead smartphone ECG for ventricular arrhythmia
Interpretation in comparison to cardiologist diagnosis.
|
Parameters |
Sensitivity (%) |
Specificity (%) |
PPV (%) |
NPV (%) |
|
Gold standard 12 Lead
ECG |
15.625 |
97.2 |
48.38 |
87.29 |
|
Smartphone Spandan ECG |
35.38 |
96.85 |
54.76 |
93.29 |
Table 4 depicts the accuracy of interpretation of ventricular arrhythmia detected by the standard ECG and smartphone ECG in comparison to the cardiologist’s diagnosis. Ventricular Arrhythmia was detected correctly in 46 (54.7%) cases and 30 (36.58%) cases by smartphone ECG and 12 lead gold standard, respectively.
Table 4: Accuracy of interpretation
of ventricular arrhythmia detected by the standard 12 lead ECG and smartphone
ECG in comparison to cardiologists’ diagnosis (n=84).
|
Parameters |
12 lead gold standard |
Smartphone ECG |
|
Ventricular Arrhythmia
detected correctly |
30 |
46 |
|
Accuracy of detection
(%) |
36.58 |
54.7 |
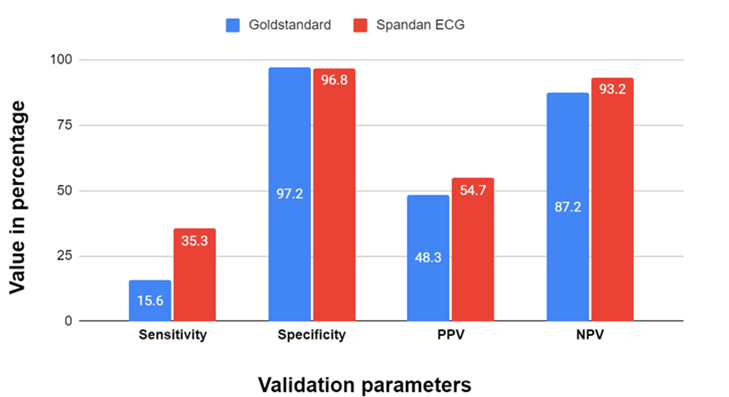
Figure 1: Validation parameters for spandan ECG and gold standard ECG in comparison to cardiologist diagnosis.
Discussion
Importantly, our cross-sectional investigation, validation study, and the single-center study showed that the smartphone ECG is capable of detecting ventricular arrhythmias utilizing a platform that is already widely accessible. This is significant because it allows electrocardiographic assessment to be expanded into new use case scenarios, such as personalized usage by the owner or point-of-care, out-of-hospital first medical contact. Situations, where a typical 12-lead ECG is not readily accessible, are among the crucial ones. Rural locations without access to healthcare, developing nations and regions, and travel settings like cruise ships and tour buses are among the settings with the greatest demand [15].
Standard 12-lead ECG equipment could not be made available in such circumstances, but the widespread use of smartphones might provide the groundwork for a wider use of electrocardiography [16]. Our research revealed a considerable deal of agreement between the spandan smartphone ECG and traditional ECG recordings for the identification of ventricular arrhythmias. When compared to simultaneously conducted traditional 12L ECG in a primary care population, the diagnostic capabilities of the 12 lead spandan smartphone ECG were shown to be good for detecting ventricular arrhythmias. To our knowledge, this is the first study to compare the smartphone-based 12-lead ECG with a cardiologist to validate the interpretation of ventricular arrhythmias.
The extended care and diagnostic capabilities for clinical decision-making and patient-facing treatment assistance are made possible by the remarkable developments in smart device technology, their downsizing (now hand-held), easy connection, and ubiquitous nature. the availability of point-of-care 12-lead ECGs taken on smart devices owned by the general public and uploaded practically instantly to a common cloud-based server present a chance to alter how healthcare is given and delivered. In order to improve access and timeliness of care, local hospitals or healthcare systems, EMS services, and communities may decide to develop and sign up for services that include monitoring, alarms, and two-way communication [17].
Our current healthcare system's approach is being outpaced by technology, so this study will determine whether a smartphone-obtained 12-lead ECG is a suitable substitute for identifying ventricular arrhythmias [18]. If this is the case, a follow-up study should evaluate the "sharing capabilities" of the smart device ECG and determine whether it can be used by non-clinicians outside of the hospital setting [19]. In a prior study using a comparable device, it was discovered that nurses were far better at ease making single lead recordings than receptionists [20]. There were several advantages to our investigation. Initially, we created a cohort generalizable to general practice by including consecutive patients who received a 12L ECG as part of standard medical practice.
The confirmation of ventricular arrhythmias detection using spandan, in contrast to other methods, enables the user's smartphone to examine ECG data in real time. The application must be installed on the user's smartphone and connected to spandan through micro USB in order for real-time monitoring to be possible. The advantage of spandan is that it is light (15 g). The device is simple to reuse since it uses swappable electrodes and a coin cell battery. This study postulates that spandan is likely to be useful in evaluating whether a patient's condition is caused by intermittent arrhythmia due to its real-time ECG monitoring. In addition, better patient compliance in using the device is predicted due to spandan's lightweight and compact size.
Conclusion
Cardiovascular illnesses have a significant negative influence on people's daily lives and their physical and emotional well-being. Hence, it's essential to frequently do ECG exams and to avoid the development of cardiovascular problems as early as possible in daily life. At this time, the professional doctor is still required to use the observation technique and this transmission to carry out the diagnosis while employing the ECG diagnostic method. While it is crucial to develop an automated arrhythmia detection algorithm, the conventional approach uses a lot of human and material resources and wastes a lot of physicians' and patients' valuable treatment time.
Nowadays, certain cardiac monitoring devices suggest offering basic arrhythmia approaches, but the diagnostic accuracy of arrhythmias is restricted due to the many devices from various manufacturers and the weak immunity of some devices to interference. The diagnostic and treatment procedure can be sped up with the help of a mobile application. An intuitive smartphone software called spandan has produced promising results in the detection of rhythmic abnormalities. The spandan ECG device scored highly for precision, sensitivity, and specificity. The total accuracy of smartphone ECG in identifying arrhythmias increased by 66.8%, or a significant growth in the accuracy of computer interpretation when compared to the diagnosis made by a cardiologist, thus mobile ECG-based devices may be employed for this purpose. So, the smartphone-based ECG would not only make life easier for primary care physicians but also improve the patient experience. According to these findings, the app may be considered for future rhythm abnormalities screening or case-finding programs. Doctors should exercise caution before acting on electrocardiographic diagnoses generated by this smartphone-based 12-lead ECG equipment.
Limitations
A single center and one device were employed in this investigation. Participants were given instructions on how to use the smartphone application before receiving each recording, and their ability to catch each trace was instantly evaluated. Without this direction, the accuracy of the recorded tracings in an ambulatory setting may decrease. Another potential drawback was that the average population age of the study was 54 years old, which was older than the average population age of Indians. Thus, it's probable that the findings don't truly represent what the whole population would go through.
Funding
Funded by Sunfox Technologies for validation of spandan ECG device.
Conflicts of Interest
None.
Ethical Approval
The study was approved by the Institutional Ethics Committee.
Consent to Participate
The written consent form was collected from the enrolled subjects.
Author Contributions
Sahil Mahajan: Principal investigator of the study and study conceptualizing. Salil Garg: Co-principal investigator of study and study protocol designing. Yogendra Singh: Interpretation of the ECG reports and data evaluation. Richa Sharma: Interpretation of the ECG reports and data evaluation. Nitin Chandola: Data statistics and research coordinator of the study. Tanuj Bhatia: Study methodology and protocol designing. Basundhara Bansal: Study trial coordinator and data management.
Article Info
Article Type
Research ArticlePublication history
Received: Tue 04, Jul 2023Accepted: Thu 03, Aug 2023
Published: Wed 16, Aug 2023
Copyright
© 2023 Nitin Chandola. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JICOA.2023.02.01
Figures & Tables
Table 1: Baseline characteristics of
the study population.
|
Parameters |
Overall patients (n=1337) |
Standard 12 Lead ECG |
12 Lead Smartphone ECG |
Cardiologist’s Diagnosis |
|
Age in years (Mean±SD)
years |
54.42±14.58 |
|||
|
Female, n(%) |
455 (34.03) |
|||
|
Male, n(%) |
881 (65.89) |
|||
|
BMI(Mean)(Kg/m2) |
24.34 |
|||
|
Chest pain |
239 |
|||
|
Palpitations |
49 |
|||
|
Shortness of breath |
94 |
|||
|
Hypertension |
87 |
|||
|
COVID-19 |
65 |
|||
|
Pacemaker implantation |
37 |
|||
|
Smoker |
141 |
|||
|
Diabetic |
204 |
|||
|
Subjects on
Anti-Coagulant Drugs |
500 |
|||
|
Subjects on Diuretics
Drugs |
234 |
|||
|
Subjects on Antacid |
293 |
|||
|
Subjects on
Anti-Hypertensive Drugs |
453 |
|||
|
Subjects on
Anti-Anginal Drugs |
123 |
|||
|
Anti-Hyperlipidemic
Drugs |
350 |
|||
|
Hyperglycimic Drugs |
75 |
|||
|
Arrhythmic ECG |
NA |
141 |
130 |
108 |
|
Non Arrhythmic ECG |
NA |
1196 |
1207 |
1229 |
Table 2: Confusion matrix of
ventricular arrhythmia detection for 12 lead standard ECG and smartphone ECG in
comparison to cardiologist diagnosis for overall evaluation.
|
Parameters |
12 lead Gold standard |
Smartphone ECG |
|
True Positive |
30 |
46 |
|
True Negative |
1113 |
1169 |
|
False Positive |
32 |
38 |
|
False Negative |
162 |
84 |
Table 3: The sensitivity,
specificity, positive predictive value (PPV), and negative predictive value
(NPV) of the standard ECG and 12 lead smartphone ECG for ventricular arrhythmia
Interpretation in comparison to cardiologist diagnosis.
|
Parameters |
Sensitivity (%) |
Specificity (%) |
PPV (%) |
NPV (%) |
|
Gold standard 12 Lead
ECG |
15.625 |
97.2 |
48.38 |
87.29 |
|
Smartphone Spandan ECG |
35.38 |
96.85 |
54.76 |
93.29 |
Table 4: Accuracy of interpretation
of ventricular arrhythmia detected by the standard 12 lead ECG and smartphone
ECG in comparison to cardiologists’ diagnosis (n=84).
|
Parameters |
12 lead gold standard |
Smartphone ECG |
|
Ventricular Arrhythmia
detected correctly |
30 |
46 |
|
Accuracy of detection
(%) |
36.58 |
54.7 |
References
1. Sanders D, Ungar L,
Eskander MA, Seto AH (2019) Ambulatory ECG monitoring in the age of
smartphones. Clevel Clin J Med, 86: 483-493. [Crossref]
2. Herrmann J (2020)
Adverse cardiac effects of cancer therapies: cardiotoxicity and arrhythmia. Nat
Rev Cardiol 17: 474-502. [Crossref]
3. Mattioli AV,
Puviani MB, Malagoli A (2020) Quarantine and Isolation during COVID‐19
outbreak: A case of online diagnosis of supraventricular arrhythmia through
telemedicine. J Arrhythm 36: 1114-1116. [Crossref]
4. Singh M, Rao R,
Gupta S (2020) KardiaMobile for ECG monitoring and arrhythmia diagnosis. Am
Fam Physician 102: 562-564. [Crossref]
5. Pranata R, Chintya
V, Raharjo SB, Yamin M, Yuniadi Y (2019) Longer diagnosis‐to‐ablation
time is associated with recurrence of atrial fibrillation after catheter
ablation-Systematic review and meta‐analysis. J
Arrhythm 36: 289-294. [Crossref]
6. Gupta V, Mittal M
(2020) A novel method of cardiac arrhythmia detection in electrocardiogram
signal. International Journal of Medical Engineering and Informatics 12:
489-499.
7. Orchard J, Lowres
N, Freedman SB, Ladak L, Lee W et al. (2016) Screening for atrial fibrillation
during influenza vaccinations by primary care nurses using a smartphone
electrocardiograph (iECG): a feasibility study. Eur J Prev Cardiol 23:
13-20. [Crossref]
8. Phillips D,
O’Callaghan P, Zaidi A (2021) Arrhythmia in an athlete diagnosed by smartphone
electrocardiogram: a case report. Eur Heart J Case Rep 5: ytab186. [Crossref]
9. Inui T, Kohno H,
Kawasaki Y, Matsuura K, Ueda H et al. (2020) Use of a smartwatch for early
detection of paroxysmal atrial fibrillation: validation study. JMIR Cardio
4: e14857. [Crossref]
10. Smisek R, Hejc J,
Ronzhina M, Nemcova A, Marsanova L et al. (2018) Multi-stage SVM approach for
cardiac arrhythmias detection in short single-lead ECG recorded by a wearable
device. Physiol Meas 39: 094003. [Crossref]
11. Strik M, Ploux S,
Ramirez FD, Abu Alrub S, Jaîs P et al. (2021) Smartwatch-based detection of
cardiac arrhythmias: Beyond the differentiation between sinus rhythm and atrial
fibrillation. Heart Rhythm 18: 1524-1532. [Crossref]
12. Samol A, Bischof K,
Luani B, Pascut D, Wiemer M et al Single-lead ECG recordings including
Einthoven and Wilson leads by a smartwatch. a new era of patient directed early
ECG differential diagnosis of cardiac diseases? Sensors (Basel) 19:
4377. [Crossref]
13. Selder JL, Breukel
L, Blok S, van Rossum AC, Tulevski II et al. A mobile one-lead ECG device
incorporated in a symptom-driven remote arrhythmia monitoring program The first
5,982 Hartwacht ECGs. Neth Heart J 27: 38-45. [Crossref]
14. Himmelreich JCL,
Karregat EPM, Lucassen WAM, van Weert HCPM, de Groot JR et al. (2019)
Diagnostic accuracy of a smartphone-operated, single-lead electrocardiography
device for detection of rhythm and conduction abnormalities in primary care. Ann
Fam Med 17: 403-411. [Crossref]
15. Kim YG, Choi JI,
Kim HJ, Min K, Choi YY et al. A Watch-Type Electrocardiography is a Reliable
Tool for Detecting Paroxysmal Cardiac Arrhythmias. J Clin Med 11: 3333.
[Crossref]
16. Casanova GB,
Sarmiento DO, Bustos MJ, Duque AO, Caicedo HA (2019) Techniques of acquisition
and processing of electrocardiographic signals in the detection of cardiac
arrhythmias. Respuestas 24: 91-102.
17. Bazi Y, Al Rahhal
MM, AlHichri H, Ammour N, Alajlan N et al. (2020) Real-time mobile-based
electrocardiogram system for remote monitoring of patients with cardiac
arrhythmias. International Journal of Pattern Recognition and Artificial
Intelligence 34: 2058013.
18. Pereira T, Tran N,
Gadhoumi K, Pelter MM, Do DH et al. Photoplethysmography based atrial
fibrillation detection: a review. NPJ Digit Med 3: 3. [Crossref]
19. Proesmans T, Mortelmans C, Van Haelst R, Verbrugge F, Vandervoort P et al. (2019) Mobile phone–based use of the photoplethysmography technique to detect atrial fibrillation in primary care: diagnostic accuracy study of the fibricheck app. JMIR Mhealth Uhealth 7: e12284. [Crossref]
20. Ding EY, Han D, Whitcomb C, Bashar SK, Adaramola O et al. (2019) Accuracy and usability of a novel algorithm for detection of irregular pulse using a smartwatch among older adults: observational study. JMIR Cardio 3: e13850. [Crossref]