Desmoplastic Ameloblastoma with Prominent Osteoplasia (Osteoplastic Ameloblastoma) as a Recurrence after 14 Years: A Case Report and Literature Review
A B S T R A C T
Background: Ameloblastoma is the most common odontogenic tumor arising from the odontogenic epithelium and is known for its distinct aggressive clinical behaviour and characteristic histologic picture. Very few cases of desmoplastic ameloblastoma with prominent osteoplasia (osteoplastic ameloblastoma) exhibiting formation of metaplastic bone trabeculae rimmed by active osteoblasts have been described.
Case Presentation: We report an interesting case of desmoplastic ameloblastoma with prominent osteoplasia (osteoplastic ameloblastoma) in a 38-year-old male presented as a recurrence after 14 years in the anterior mandible.
Conclusion: A hybrid lesion of desmoplastic ameloblastoma with osteoplastic pattern (osteoplastic ameloblastoma) needs inclusion of new cases to understand their behaviour. Recurrence of lesion after 14 years of initial surgery in our case presents the importance of regular bi-annual follow-up for lifetime.
Keywords
Ameloblastoma, desmoplasia, osteoplasia, odontogenic tumor, transforming growth factor-β
Introduction
Ameloblastoma is the most common locally aggressive benign odontogenic epithelial tumor of the jaw bones, mainly affecting the posterior mandible [1]. Follicular and plexiform are the main histological variants. Histomorphologic subtypes of the above two main patterns are basaloid, acanthomatous, granular cell, unicystic and more recently, clear cell, papilliferous, kerato-variant and desmoplastic ameloblastoma [2]. Desmoplastic ameloblastoma with prominent osteoplasia (osteoplastic ameloblastoma) may be defined as a benign but locally invasive variant consisting of proliferating, irregular, often bizarrely shaped islands and cords of odontogenic epithelium of varying sizes embedded in a desmoplastic connective tissue stroma accompanied by formation of metaplastic bone trabeculae (osteoplasia) rimmed by active osteoblasts [3]. We report an interesting case of desmoplastic ameloblastoma with prominent osteoplasia (osteoplastic ameloblastoma) of the mandible occurring as a recurrence after 14 years.
Case Presentation
A 38-year-old male reported to our department with a chief complaint of gradually increasing painless swelling in the mandibular anterior region for 4 years. Patient gave past history of operation 14 years back for removal of similar lesion. He has lost all the previous hospital records due to continuous shifting. His medical, social and family history was non-contributory. Extra-oral examination revealed a single, ovoid, well-circumscribed swelling measuring about 7 cm x 5 cm in size in the mandibular anterior region involving the chin (Figure 1). The lesion extended superior-inferiorly from the left angle of mouth involving inferior border of the mandible. No evidence of draining sinus, pus discharge or cervical lymphadenopathy was observed. The overlying skin was normal. On palpation the swelling was bony hard, non-tender, with intact overlying mucosa.

Figure 1: Extra-oral view showing a well-circumscribed solitary swelling in the mandibular anterior region.
Intra-orally, the swelling extended from the mid-line to the distal surface of permanent mandibular right second premolar obliterating the right mandibular labial vestibule. No evidence of paresthesia was observed. An edentulous area extending from the permanent mandibular right canine to permanent mandibular left second molar was noted. Oral hygiene of the patient was fair (Figure 2). The panoramic radiograph demonstrated a well-defined multilocular mixed radiolucent and radio-opaque appearance extending from left parasymphysis to distal of permanent mandibular right second premolar. Presence of well-defined radio-opacity in shape of wires was noted in the mandibular anterior region suggesting previous operation (Figure 3).

Figure 2: Intra-oral view showing obliteration of right mandibular labial vestibule with partial edentulism.
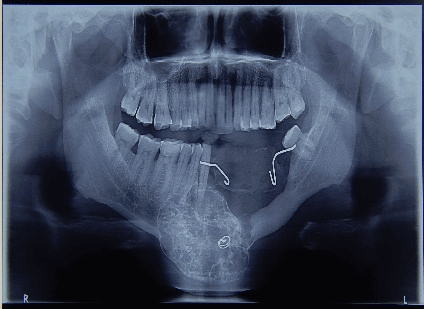
Figure 3: Panoramic radiograph showing well-defined mixed radio-lucent and radio-opaque appearance in the mandibular anterior region.
Cone-beam computed tomography presented a roughly ovoid lesion with altered trabecular pattern observed superiorly from mid-root level of permanent right mandibular canine and extending below the inferior border of mandible, located in the mandibular anterior region. Bicortical expansion of the lesion was also noted (Figure 4). A provisional diagnosis of recurrent ameloblastoma was considered. However benign fibro-osseous lesion was also kept in mind as a differential diagnosis. Incisional biopsy was performed under local anaesthesia and subjected to histopathological examination. Microscopic examination of hematoxylin and eosin stained section presented an interesting finding of numerous areas of new bone formation rimmed by plump osteoblasts distributed evenly throughout the desmoplastic stroma. Differentiation of mesenchymal cells into osteoblasts and formation of new trabecular bone was also noted. The diagnosis of desmoplastic ameloblastoma with osteoplasia (osteoplastic ameloblastoma) was made (Figure 5).

Figure 4: Cone beam computed tomography showing altered trabecular pattern and bicortical expansion of the lesion.

Figure 5: Photomicrograph showing animal face-like pattern of ameloblastic island in a desmoplastic stroma (H&E stain, original magnification x10).
Segmental resection of the ameloblastoma from the mandibular anterior region was then performed under general anaesthesia (Figure 6). On gross examination the cut surface of the specimen appeared hard and gritty in texture (Figure 7A). Histopathological diagnosis of the excised specimen was consistent with the incisional diagnosis of desmoplastic ameloblastoma with prominent osteoplasia (osteoplastic ameloblastoma). Postoperative healing was uneventful. The patient has been followed up for one year without any evidence of recurrence.

Figure 6: Gross specimen of segmental resection of the mandible. Inset showing gross specimen radiograph exhibiting mixed radio-lucent and radio-opaque appearance in the mandibular anterior region.
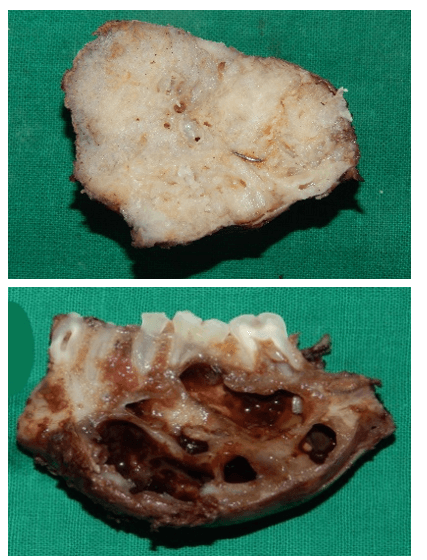
Figure 7: A) Gross specimen of desmoplastic ameloblastoma with prominent osteoplasia (osteoplastic ameloblastoma) showing whitish hard gritty cut surface. B) Gross specimen of conventional ameloblastoma showing multicystic appearance.
Discussion
Desmoplastic ameloblastoma was first described in detail by Eversole et al. in 1984 and may be defined as a variant of ameloblastoma with specific clinical, imaging and histological features [4]. Previous reported cases of desmoplastic ameloblastoma have shown this variant to have a strong predilection for the anterior premolar region of the jaws, occurring with equal frequency in the maxilla and mandible, in contrast to other variants of conventional ameloblastoma, which are more common in the posterior mandible [5]. It presents with a unique radiographic appearance resembling fibro-osseous lesions and shows distinct histopathology characterized by extensive stromal collagenisation or desmoplasia surrounding compressed islands of odontogenic epithelium [6-10].
In 2005, ameloblastoma were sub-divided into the solid/multicystic type, extraosseous/peripheral type, desmoplastic type and unicystic type [10]. This sub-classification was regarded as too complex and lacking in behavioural or biological significance. The new classification has dropped the terminology desmoplastic ameloblastoma and described it as a histological variant of conventional ameloblastoma. Like other variants, including follicular, plexiform and acanthomatous, they are histologically distinctive and can be described, but as a diagnostic entity, there is no evidence of any differences in behaviour [1]. Bone formed by the osteoplastic activity of tumor cells resembles the bone formed in desmoplasia. The stimuli to stromal fibroblasts for desmoplasia may also result in the differentiation of the stromal mesenchymal cells into osteoblasts and thus causing osteoplasia [11]. Present case also exhibited desmoplasia with prominent osteoplasia and hence diagnosed as desmoplastic ameloblastoma with prominent osteoplasia (osteoplastic ameloblastoma).
Present case demonstrated a difference in the appearance of gross specimen when compared to that of a conventional ameloblastoma. On gross examination, our case presented a hard and gritty textured cut surface lacking cystic degeneration (Figure 7A) against multicystic appearance of conventional ameloblastoma (Figure 7B). Histopathologically, the present case revealed desmoplasia with prominent osteoplasia, showing metaplastic bony trabeculae containing osteocytes lined by plump active osteoblasts. Remnants of non-neoplastic bone in the tumor tissue, thus suggest that the signals for desmoplasia could also be involved in the transformation of mesenchymal cells into active osteoblasts and thus forming new bone (osteoplasia) [12].
Interestingly, there have been two studies that have described intensive nuclear expression of Transforming growth factor-β (TGF-β) in the areas of desmoplastic ameloblastoma in hybrid lesions. Fibroblasts in highly collagenised stroma often showed light to moderate TGF- β positivity [12, 13]. TGF- β is involved in synthesis of extracellular matrix like collagen, fibronectin, proteoglycans and other. It is also involved in inhibition of degradation of ECM by an inhibitory action and a stimulatory action. The inhibitory action of TGF- β is mediated by production of matrix metalloproteins whereas the stimulatory action activates the enzyme inhibitors. TGF- β when applied to bone site shows enhanced bone but it was also seen that it exhibited diffused effects on an osteoblastic cell proliferation and differentiation depending on its or maturation stage of osteoblasts [13]. The plausible explanation for prominent osteoplasia in the reported case could be due to bone formation over long term and presented after all these years.
Extensive search on PubMed found only seven reported cases of desmoplastic ameloblastoma with prominent osteoplasia (osteoplastic ameloblastoma) [11, 12, 14-17]. The review of reported cases showed the age range for desmoplastic ameloblastoma with prominent osteoplasia to be 31-64 years with a slight male predilection. Radiographically, majority of the reviewed cases demonstrated multilocular mixed radio-lucent and radio-opaque appearance mimicking fibro-osseous lesion. The distribution of desmoplastic ameloblastoma with prominent osteoplasia was seen in the anterior maxilla in five cases and remaining two in the anterior mandible. We presented a case of desmoplastic ameloblastoma with prominent osteoplasia (osteoplastic ameloblastoma) in a 38-year-old male in the anterior mandible presented as a recurrence after 14 years, showing a multilocular mixed radio-lucent and radio-opaque appearance.
Conclusion
A hybrid lesion of desmoplastic ameloblastoma with osteoplastic pattern (osteoplastic ameloblastoma) needs inclusion of new cases to understand their behaviour. Recurrence of lesion after 14 years of initial surgery in our case presents the importance of regular bi-annual follow-up for lifetime.
Acknowledgement
Not applicable.
Conflicts of Interest
None.
Financial Disclosure
None.
Funding
None.
Availability of Data and Materials
All data generated or analysed during this study are included in this published article.
Ethical Approval and Consent to Participate
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Competing Interests
None.
Abbreviations
TGF-β: Transforming growth factor-β
Article Info
Article Type
Case Report and Review of the LiteraturePublication history
Received: Sat 23, May 2020Accepted: Tue 09, Jun 2020
Published: Thu 25, Jun 2020
Copyright
© 2023 Rajiv S. Desai. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.06.20
Figures & Tables
References
- Speight PM, Takata T (2018) New tumour entities in the 4th edition of the World Health Organization Classification of Head and Neck tumours: odontogenic and maxillofacial bone tumours. Virchows Arch 472: 331-339. [Crossref]
- Waldron CA, el Mofty SK (1987) A histopathologic study of 116 ameloblastomas with special reference to the desmoplastic variant. Oral Surg Oral Med Oral Pathol 63: 441-451. [Crossref]
- Savithri V, Janardhanan M, Suresh R, Kumar RV (2013) Desmoplastic ameloblastoma with osteoplasia: Review of literature with a case report. J Oral Maxillofac Pathol 17: 298-301. [Crossref]
- Eversole LR, Leider AS, Hansen LS (1984) Ameloblastoma with pronounced desmoplasia. J Oral Maxillofac Surg 42: 735-740. [Crossref]
- Sivapathasundharam B, Einstein A, Syed RI (2007) Desmoplastic ameloblastoma in Indians: Report of five cases and review of literature. Indian J Dent Res 18: 218-221. [Crossref]
- Kishino M, Murakama S, Fukuda Y, Ishida T (2001) Pathology of desmoplastic ameloblastoma. J Oral Pathol Med 30: 35-40. [Crossref]
- Beckley ML, Farhood V, Helfend LK, Alijanian A (2002) Desmoplastic ameloblastoma of the mandible: a case report and review of the literature. J Oral Maxillofac Sur 60: 194-198. [Crossref]
- Sun ZJ, Wu YR, Cheng N, Zwahlen RA, Zhao YF (2009) Desmoplastic ameloblastoma-a review. Oral Oncol 45: 752-759. [Crossref]
- Sakashita H, Miyata M, Okabe K, Kurumaya H (1998) Desmoplastic ameloblastoma in the maxilla: a case report. J Oral Maxillofac Surg 56: 783-786. [Crossref]
- Gardner DG, Heikinheimo K, Shear M, Philipsen HP, Coleman H (2005) Ameloblastomas. In: Barnes L, Eveson JW, Reichart P, Sidransky D World health organization classification of tumours. Pathology and genetics of head and neck tumours, IARC Press, Lyon 296-300.
- Philipsen HP, Ormiston IW, Reichart PA (1992) The desmo- and osteoplastic ameloblastoma. Histologic variant or clinicopathologic entity? Case reports. Int J Oral Maxillofac Surg 21: 352-357. [Crossref]
- Angadi PV, Kale A, Hallikerimath S, Kotrashetti V, Mane D et al. (2011) 'Hybrid' desmoplastic ameloblastoma: an unusual case report with immunohistochemical investigation for TGF-β and review of literature. Eastern J Med 16: 9-17.
- Takata T, Miyauchi M, Ogawa I, Kudo Y, Takekoshi T et al. (2000) Immunoexpression of Transforming Growth Factor Beta in Desmoplastic Ameloblastoma. Virchows Arch 436: 319-323. [Crossref]
- Thompson IO, van Rensburg LJ, Phillips VM (1996) Desmoplastic ameloblastoma: correlative histopathology, radiology and CT-MR imaging. J Oral Pathol Med 25: 405-410. [Crossref]
- Iida S, Kogo M, Kishino M, Matsuya T (2002) Desmoplastic Ameloblastoma With Large Cystic Change in the Maxillary Sinus: Report of a Case. J Oral Maxillofac Surg 60: 1195-1198. [Crossref]
- Itoh Y, Nakahara H, Itoh R, Ito A, Satou T (2012) Osteoplastic ameloblastoma: A case report and literature review. Oral Surg Oral Med Oral Pathol Oral Radiol 113: e23-e28. [Crossref]
- Okada Y, Sugimura M, Ishida T (1986) Ameloblastoma accompanied by prominent bone formation. J Oral Maxillofac Surg 44: 555-557. [Crossref]