Enterolithotomy for Gallstone Ileus: An Uncommon Cause of Intestinal Obstruction
A B S T R A C T
Gallstone ileus is a rare complication of cholelithiasis which represent 1-3% of the causes of intestinal obstruction in the general population and is more commonly seen in females. Gallstone ileus does not present with unique symptoms, making the diagnosis difficult. Symptoms are often non-specific with intermittent intestinal obstruction. The management is surgical, but there is no consensus as to which of the different surgical techniques is the procedure of choice. We report an interesting case of a 78-year-old male brought to casualty with abdominal pain following a history of fall. Managed as a case of blunt trauma abdomen initially. Surprisingly investigations showed features of small bowel obstruction, a hyperdense structure in the distal jejunum with dilated proximal jejunal loops suggestive of gallstone ileus. The patient had undergone exploratory laparotomy with enterotomy and removal of gallstones without any postoperative complications. Intraoperatively cholecystoduodenal fistula was identified and the patient was electively planned for cholecystectomy and fistula repair.
Keywords
Gallstone ileus, small bowel obstruction, choledochoduodenal fistula
Introduction
Gallstone ileus is a gallstone-induced mechanical obstruction of the small bowel and is a rare complication of cholelithiasis [1]. Gallstone ileus itself is a misnomer as the underlying pathology is that of mechanical obstruction of the bowel by a gallstone rather than a paralytic ileus as the name suggests [2]. It accounts for 1-4% of all cases of mechanical intestinal obstruction, but up to 25% of the cases are comprised of patients over 65 years of age [3-6]. The average age of presentation is 74 years. These patients are usually elderly, frail, and with multiple comorbidities. Gallstone ileus is more prevalent in women than men (ratio of 1:3-7) [2, 7-10]. The morbidity and mortality of gallstone ileus remain remarkably high, most likely due to misdiagnosis and delayed diagnosis [11]. Early diagnosis and prompt treatment are mandatory for a successful outcome. We report a rare case of a 78-year-old male diagnosed with gallstone-induced mechanical small bowel obstruction who presented to us with acute abdominal pain following blunt trauma to the abdomen which made the diagnosis more challenging.
Case Report
A 78-year-old male patient presented to the emergency department with abdominal pain and vomiting, following a history of falls while traveling on the bus. The patient was diabetic, hypertensive and asthmatic on treatment. At the time of presentation, the vitals were stable with a pulse rate of 74/minute, blood pressure of 140/90mmHg and oxygen saturation of 97% in room air. On examination, the abdomen was distended (Figure 1), and diffusely tender with guarding. He was treated as a case of blunt trauma abdomen with serial monitoring of pulse rate, blood pressure, saturation, urine output, and haemoglobin. Initial blood investigations were normal. Liver enzymes were normal.

Figure 1(A & B): 78-year-old male with blunt trauma abdomen with features of abdominal distension-initial presentation in an emergency.
An abdominal erect x-ray was taken and surprisingly it showed multiple hyperdense foci in multiple quadrants in of abdomen (Figure 2). The patient became asymptomatic after one day of conservative management by keeping nil per oral and intravenous analgesics. Ultrasound of the abdomen revealed only bilateral raised renal echoes and there was no evidence of solid organ injury.

Figure 2: Multiple hyperdense foci in multiple quadrants of abdomen.
On day 3 of admission, oral soft feeds were initiated. On the same day, the patient developed abdominal distension with diffuse abdominal pain. Repeating an abdominal erect x-ray revealed a hyperdense focus more prominently in the left iliac fossa with dilatation of small bowel loops with multiple air-fluid levels making us suspect gallstone ileus (Figure 3).

Figure 3: Hyperdense foci more predominant in the left iliac fossa.
We proceeded for further imaging with CECT abdomen revealing mild free fluid noted in the pelvis, peri splenic and left paracolic gutter. Hyperdense structure measuring 2.4 × 2.30 cm of average HU750 with hypodense center noted in the distal jejunum (Figure 4). Proximal to it jejunum appears dilated measuring 3.1 cm in diameter with adjacent fat stranding. Distal bowel loops appear collapsed. The common bile duct was normal. Gall bladder appears contracted with no evidence of calculus. There was no solid organ injury.

Figure 4: Hyperdense structure measuring 2.4 × 2.30 cm of average HU750 with hypodense center noted in the distal jejunum.
The patient was posted for emergency exploratory laparotomy. Enterotomy was placed at the distal ileum at the antimesenteric border 10 cm proximal to the site of gallstone impaction and gall stone was milked and delivered through the enterotomy site (Figure 6). The enterotomy was primarily repaired with 3-0 vicryl and 3-0 silk. The gall bladder was contracted with suspicious communication with the first part of the duodenum suggesting a cholecystoduodenal fistula (Figure 5). There was an intense inflammatory process in the right upper quadrant as well. Since the patient is old and his physiologic status may not permit him to proceed with cholecystectomy and fistula repair in this emergent setting, only enterotomy and stone extraction was done in this setting. The postoperative period was uneventful. The patient was planned for cholecystectomy and fistula closure at a later date.
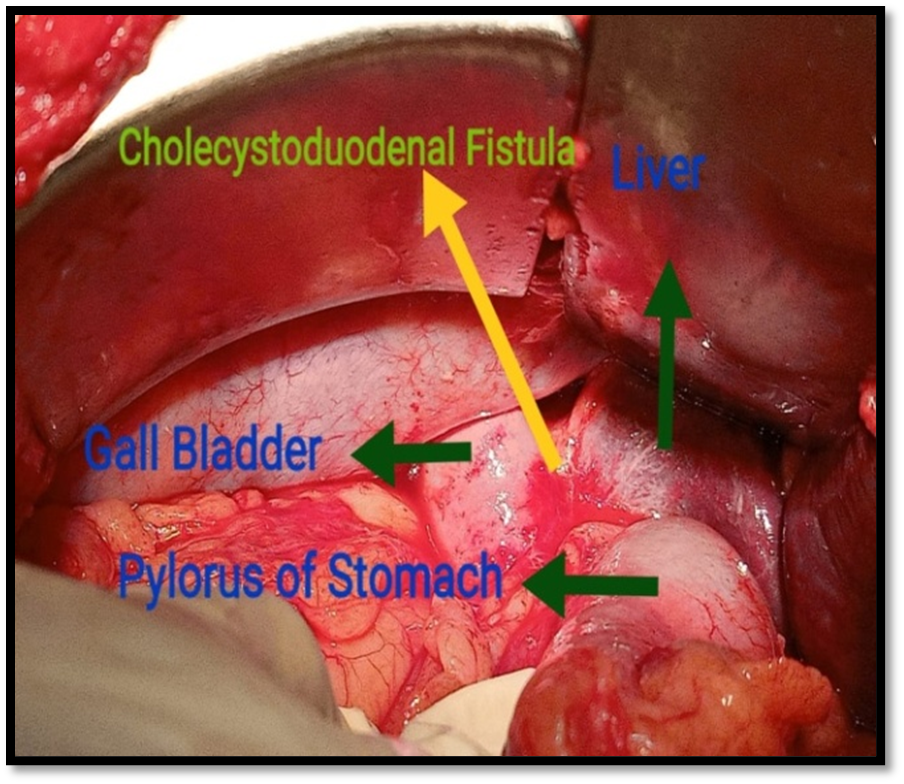
Figure 5: Intraoperative image of cholecystoduodenal fistula.
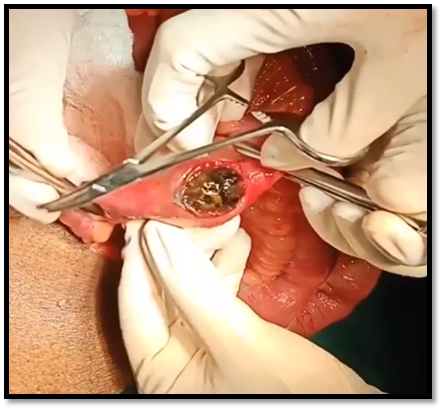
Figure 6: Intraoperative image of gallstone extraction.
Discussion
Gallstone ileus is a rare complication of gallstone disease with variable and non-specific clinical presentation. It requires a high index of suspicion, particularly in elderly patients presenting with signs of small bowel obstruction [12]. The most common sites of impaction are the ileum (50-60.5%), jejunum (16.1-26.9%), duodenum (3.5-14.6%), and colon (3-4.1%) [2, 5]. Mechanical intestinal obstruction with abdominal pain and vomiting is the most common clinical presentation as seen in 80 per cent of our patients. Proximal obstruction is characteristically accompanied by bilious vomiting and gastric dilatation, whereas feculent vomiting and bowel distension are often prominent in ileal or sigmoid obstruction [2].
The presence of cholecystoenteric fistula is a usual finding in gallstone ileus. Although not seen in the case presented, the majority of the cases that present have a previous history of acute cholecystitis resulting in the formation of cholecystoenteric fistula. During acute cholecystitis, pericholecystic inflammation causes adhesions between the gall bladder and gastrointestinal tract, most commonly the duodenum due to its proximity. The pressure effect of the gallstone on the gall bladder wall causes pressure necrosis forming the fistulous tract [13, 14]. The formation of a biliary-enteric fistula allows the entry of gallstones into the gastrointestinal system and complicates 0.3%-1.5% of cases of cholelithiasis [5].
Although symptoms of gallstone ileus are non-specific, it usually occurs in older women with a classical episodic subacute intestinal obstruction known as ‘tumbling obstruction’ which occurs as the stone tumbles through the intestinal lumen causing multiple episodes of subacute obstruction, which gets relieved spontaneously until the finally gets impacted usually in the distal ileum or ileocecal valve causing more profound feature of obstruction. So clinicians can get a vague picture of symptoms even days before the patient presents to him/her. On examination, the patient may be febrile and appears dehydrated, with abdominal signs including abdominal distention, and increased bowel sounds [2]. The biochemical parameters are also non-specific but may show leucocytosis and electrolyte imbalance due to dehydration and raised aminotransferase levels [2].
Rigler’s triad describes classical features seen on imaging suggestive of gallstone ileus: intestinal obstruction, pneumobilia, gallstone within the intestinal lumen and, more recently, a change in position of the gallstone on serial imaging [15]. CT scan of the abdomen with a sensitivity and specificity of 93% and 100% respectively is considered the gold standard [16]. Plain abdominal films are usually nonspecific because significant calcification of the stone is necessary for it to be visualized radiographically. Abdominal USG is useful to confirm the presence of cholelithiasis and may identify a fistula if present [17].
There are usually 3 different methods in the management of gallstone ileus: enterolithotomy alone, enterolithotomy coupled with cholecystectomy and fistula closure (one-stage procedure), enterolithotomy then delayed cholecystectomy at a later time, usually 4-6 weeks (two-stage procedure) [18]. Of the three procedures, there is a small increased risk of morbidity and mortality associated with a single-stage procedure; however, there is also a known risk of further complications from gallstones while awaiting a cholecystectomy and repair of fistula in a two-stage procedure
Conclusion
Gallstone ileus, being a rare complication of gallstone disease often presenting with non-specific signs and symptoms, needs a high index of suspicion for early diagnosis and prompt management. The morbidity and mortality of gallstone ileus remain remarkably high, most likely due to misdiagnosis and delayed diagnosis.
Conflict of Interests
None.
Funding
None.
Ethical Approval
Not required.
Article Info
Article Type
Case ReportPublication history
Received: Sat 17, Jun 2023Accepted: Mon 10, Jul 2023
Published: Sat 15, Jul 2023
Copyright
© 2023 Ajil Antony. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JSCR.2023.03.02
Figures & Tables
References
1.
Abou Saif A, Al
Kawas FH (2002) Complications of gallstone disease: Mirizzi syndrome,
cholecystocholedochal fistula, and gallstone ileus. Am J Gastroenterol
97: 249-254. [Crossref]
2.
Ploneda Valencia
CF, Gallo Morales M, Rinchon C, Navarro Muñiz E, Bautista López CA et al.
(2017) Gallstone ileus: An overview of the literature. Rev Gastroenterol Mex
82: 248-254. [Crossref]
3.
Kurtz RJ, Heimann
TM, Kurtz AB (1983) Gallstone ileus: A diagnostic problem. Am J Surg
146: 314-317. [Crossref]
4.
Clavien PA, Richon
J, Burgan S, Rohner A (1990) Gallstone ileus. Br J Surg 77: 737-742. [Crossref]
5.
Reisner RM, Cohen
JR (1994) Gallstone ileus: a review of 1001 reported cases. Am Surg 60:
441-446. [Crossref]
6.
Hermosa JI, Cazador
AC, Vilà JG, García JR, Francesch M et al. (2001) Gallstone Ileus: results of
analysis of a series of 40 patients. Gastroenterol Hepatol 24: 489-494.
[Crossref]
7.
Mallipeddi MK,
Pappas TN, Shapiro ML, Scarborough JE (2013) Gallstone ileus: revisiting
surgical outcomes using National Surgical Quality Improvement Program data. J
Surg Res 184: 84-88. [Crossref]
8.
Sahsamanis G,
Maltezos K, Dimas P, Tassos A, Mouchasiris C (2016) Bowel obstruction and
perforation due to a large gallstone. A case report. Int J Surg Case Rep
26: 193-196. [Crossref]
9.
Martín Pérez J,
Delgado Plasencia L, Bravo Gutiérrez A, Burillo Putze G, Martínez Riera A
(2013) et al. Gallstone ileus as a cause of acute abdomen. Importance of early
diagnosis for surgical treatment. Cir Esp 91: 485-489. [Crossref]
10.
Chuah PS, Curtis J,
Misra N, Hikmat D, Chawla S (2017) Pictorial review: the pearls and pitfalls of
the radiological manifestations of gallstone ileus. Abdom Radiol (NY)
42: 1169-1175. [Crossref]
11.
Lobo DN, Jobling
JC, Balfour TW (2000) Gallstone ileus: diagnostic pitfalls and therapeutic
successes. J Clin Gastroenterol 30: 72-76. [Crossref]
12.
Chang L, Chang M,
Chang HM, Chang AI, Chang F (2018) Clinical and radiological diagnosis of
gallstone ileus: a mini-review. Emerg Radiol 25: 189-196. [Crossref]
13.
Nuño Guzmán Carlos,
Marín Contreras ME, Figueroa Sánchez M, Corona JL (2016) Gallstone ileus,
clinical presentation, diagnostic and treatment approach. World J
Gastrointest Surg 8: 65-76. [Crossref]
14.
Verma A, Moonat A,
Lo A (2010) An uncommon aetiology of small bowel obstruction: gallstone ileus. J
Hosp Med 5: E21-E2. [Crossref]
15.
Rigler LG, Borman
CN, Noble JF (1941) GALLSTONE OBSTRUCTION: PATHOGENESIS AND ROENTGEN
MANIFESTATIONS. J Am Med Assoc 117: 1753-1759.
16.
Yu CY, Lin CC, Shyu
RY, Hsieh CB, Wu HS et al. (2005) Value of CT in the diagnosis and management
of gallstone ileus. World J Gastroenterol 11: 2142-2147. [Crossref]
17.
Lasson A, Lorén I,
Nilsson A, Nirhov N, Nilsson P (1995) Ultrasonography in gallstone ileus: a
diagnostic challenge. Eur J Surg 161: 259-263. [Crossref]
18. Hussain J, Alrashed AM, Alkhadher T, Wood S, Behbehani AD et al. (2018) Gall stone ileus: Unfamiliar cause of bowel obstruction. Case report and literature review. Int J Surg Case Rep 49: 44-50 [Crossref]
19. Morosin T, De Robles MSB, Putnis S (2020) Gallstone ileus: An unusual cause of intestinal obstruction. Cureus 12: e7284. [Crossref]