Femoral Hernia Presenting as Richter’s Variant: A Rare Case Report
A B S T R A C T
Background: Richter's hernia occurs when a portion of the anti-mesenteric border of a bowel wall is captured within the hernia sac, resulting in ischaemia, gangrene, and perforation. Only part of the circumference of the bowel wall is involved in Richter's hernia, which causes strangulation without obstruction. Femoral hernia presenting as a Richter’s hernia is rare.
Aim: This is to report a case of Richter’s hernia in a femoral hernia occurring in an adult female.
Case Report: In this case, a 62-year-old woman presented with a history of sudden generalized abdominal pain. Before the presentation, she had a six-year history of reducible left inguino-labial swelling that became irreducible two weeks ago. Pallor was present. Her temperature was 39.2°C, her pulse rate was 112 per minute, and her blood pressure was 132/62 mmHg. A diagnosis of a left femoral hernia was made. She was revived, and the groin swelling was explored through a midline incision over the abdomen. There was ischaemia of the anti-mesenteric border of the ileum, along with strangulated preperitoneal fat. The bowel vascularity over the anti-mesenteric border was doubtful, so a resection anastomosis of the segment of the bowel was done followed by a reduction of the bowel loop and herniorraphy.
Conclusion: It is rare for a femoral hernia to present with a Richter's hernia, but it can happen even in the absence of obstructive symptoms. Any time there is groin swelling, it is important to get a quick, correct diagnosis and treatment. If there is a delay in identification and treatment, a spontaneous faecal fistula, an uncommon complication, may develop. The relevant authorities must address this as it reflects the status of healthcare in the developing world.
Keywords
Femoral hernia, richters hernia, inguinal swelling, intestinal obstruction, anastomosis
Introduction
The German surgeon August Gottlieb Richter provided the first description of this form of hernia in 1778 and is named after him as Richter's hernia [1]. It is a rare disorder, wherein only a portion of the intestinal wall is entrapped within the hernial sac, causing ischaemia, gangrene, and perforation of the hollow viscus [1]. The femoral ring is the most frequent location of its occurrence [2]. Because of its early, deceptive presentation, propensity for early strangulation, and lack of obstructive symptoms, it may take longer to diagnose leading to an increased mortality rate [2]. If ignored this can lead disastrous complications such as spontaneous enterocutaneous fistula.
Case Report
A 62 year old lady presented with abdominal pain of severe intensity for two days associated with non passage of stools and flatus. On examination, she was haemodynamically stable. Abdomen was found to be diffusely tender with mild distension. There was an irreducible mass in the left groin below and lateral to pubic tubercle which was tender. With the clinical diagnosis of obstructed femoral hernia. Erect abdominal radiograph was done which showed features of small bowel obstruction (as shown in Figure 1). Patient was planned for emergency surgery. Intraoperatively a femoral Richter’s hernia involving a segment of the ileum was noted (Figure 2). A portion of the circumference of the bowel wall was ischaemic (Figure 3). The involved segment was resected and end to end anastomosis with herniorraphy was done. Post operative period was uneventful and patient recovered with no complications. Patient was discharged in pod 6 and is on regular follow up.
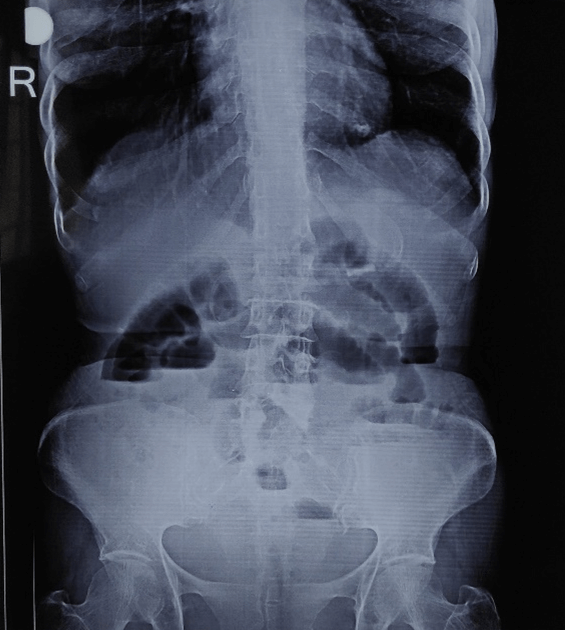
Figure 1: Pre-operative radiograph showing features suggestive of small bowel obstruction.
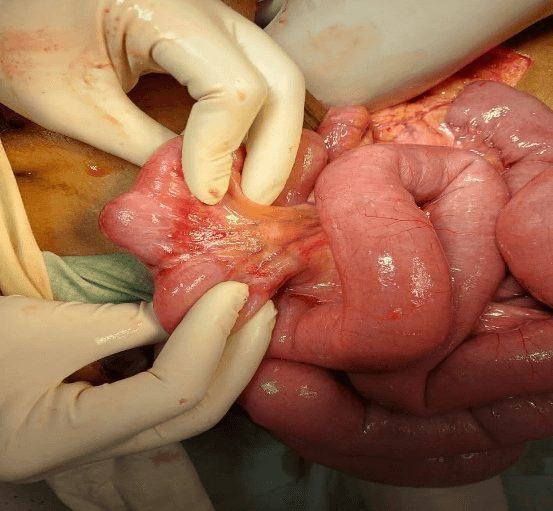
Figure 2: Intraoperative image showing Richter’s hernia.
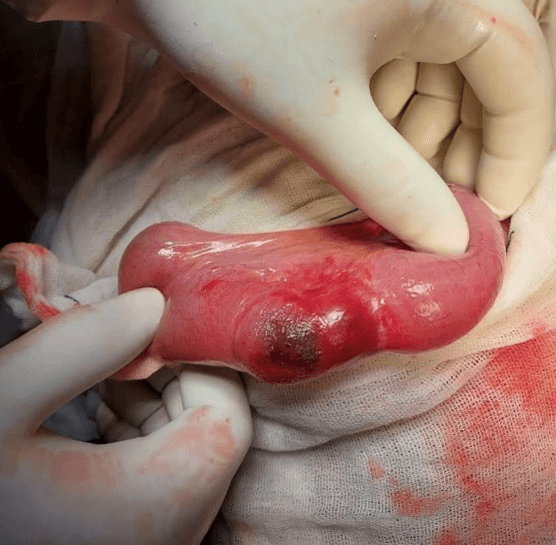
Figure 3: Intraoperative picture showing a part of the circumference of bowel wall having ischaemia.
Discussion
Fabricius Hildanus described the oldest documented instance of a Richter's hernia in 1598 [3]. With a quick assessment of the literature, Singh et al. described a rare case of spontaneous inguinal faecal fistula as a side effect of incarcerated Richter's hernia [4]. Small hernial rings big enough to entrap a portion of the intestinal wall are the hallmark of Richter's hernia. The femoral ring is the most frequent site of occurrence of Richter’s hernia (72-88%), followed by the inguinal canal (12-24%) and abdominal wall incisional hernias (4-25%). At the sites of laparoscopic port insertion, several cases have been recorded [5]. Any part of the intestine can become incarcerated, although as seen in our case, the distal ileum is most frequently affected, followed by the caecum and sigmoid colon [2]. Because only a small portion of the intestine is affected, luminal continuity is preserved, resulting in a partial intestinal obstruction with few visible clinical symptoms and signs [2]. The clinical presentation of Richter’s hernia can be divided into 3 groups.
The first is the obstructive category, which includes nausea, vomiting, peritonitis, and constipation and can cause shock if left untreated. The second group is an enterocutaneous fistula-causing strangulation with necrosis and perforation known as the post-necrotic group. Patients with limited abdominal symptoms are included in the third category, which is considered risky [6]. Due to a delay in diagnosis, this group has the highest morbidity and mortality rates.
In an untreated Richter's hernia, strangulation occurs rapidly. Reviewing 146 strangulated hernias 45 (30.8%) of them were Richter's hernias, only 25 (24.8%) of the remaining 101 patients with strangulated hernias showed intestinal necrosis, compared to 31 (68.9%) of the 45 patients who had Richter’s hernias [7]. This demonstrates how quickly Richter's hernias leads to strangulation of the bowel.
To prevent the dreaded complications, immediate surgical exploration involving intestinal resection and end-to-end anastomosis is required. Although there are many views on the strategy for surgical exploration in the literature, the access or route of the surgery is typically depending on the patient. The likelihood of a perforated parietal hernia should always be considered in necrotizing inflammations of the inguinal and vulvar regions, according to Bätz et al., even if there are no abdominal signs or symptoms [8]. Since intestinal patency is often maintained, limiting extension into the abdominal cavity also occurs as a result of a constricted hernial aperture. Midline laparotomy is also an option to evaluate the bowel status. Having a high index of clinical suspicion and judgement regarding the varied presentations of Richter’s hernia is required to have a favourable outcome in terms of reduced mortality and morbidity rates.
Conclusion
One cannot overstate the importance of receiving an early and accurate diagnosis, followed by fast treatment, in the case of any groin swelling. Prompt surgery after becoming aware of complications like irreducibility and strangulation helps prevent complications such as obstruction and strangulation. Femoral hernia with Richter’s hernia is a rare phenomenon mostly arising due to a narrow of the neck of the hernial sac preventing the entire bowel wall from herniating.
Conflicts of Interest
None.
Funding
None.
Article Info
Article Type
Case ReportPublication history
Received: Fri 07, Jul 2023Accepted: Tue 25, Jul 2023
Published: Thu 03, Aug 2023
Copyright
© 2023 Soumith Subhash. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JSCR.2023.03.04
Figures & Tables
References
1. Faridi SH, Siddiqui
B, Khan MA, Anees A, Ali SA (2013) Suprapubic Fecal Fistula Due To Richter's
Inguinal Hernia: A Case Report and Review of Literature. Iran J Med Sci
38: 129-131. [Crossref]
2. Mou CY, Lu HE, Yen
SJ, Su CJ, Tan KH et al. (2000) Richter’s hernia: report of six cases. J Med
Sci 20: 201-206.
3. Steinke W,
Zellweger R (2000) Richter’s hernia and Sir Frederick Treves: an original
clinical experience, review, and historical overview. Ann Surg 232:
710-718. [Crossref]
4. Ah KS, Moudgil A,
Aggarwal K, Sharma C, Singh K (2015) A rare case of spontaneous inguinal faecal
fistula as a complication of incarcerated Richter’s hernia with a brief review
of literature. BMC Surg 15: 67. [Crossref]
5. Boughey JC,
Nottingham JM, Walls AC (2003) Richter’s hernia in the laparoscopic era: four
case reports and review of the literature. Surg Laparosc Endosc Percutan
Tech 13: 55-58. [Crossref]
6. Gillespie RW, Glas
WN, Musselman M (1956) Richter’s hernia. Arch Surg 73: 590.
7. Horbach JM (1986) Invagination for Richter-type strangulated hernias. Trop Doct 16: 163-168. [Crossref]
8. Bätz W, Dzieniszewski GP, Neher M (1984) Necrotizing inflammation of the vulva-a symptom of Richter intestinal wall hernia. Geburtshilfe Frauenheilkd 44: 518-520. [Crossref]