Foreign Body Reaction with Granuloma 10 Years After Achilles Tendon Reconstruction with the LARS Ligament
A B S T R A C T
Achilles tendon rupture is one of the most common tendon injury in adult population. Synthetic ligament has been an attractive alternative for reconstruction chronic Achilles tendon tears. Ligament reconstruction with the LARS ligament has been a popular choice owing to its low-complication rates. LARS ligament is a non-absorbable synthetic ligament device. There are no long-term results of LARS ligament reconstruction for Achilles tendon reconstruction in literature. We describe a successful management of foreign body granuloma in a LARS ligament Achilles tendon graft and a technique to reconstruct the tendon following its excision.
Keywords
LARS ligament, Achilles tendon reconstruction, granuloma
Introduction
Achilles tendon (AT) is largest tendon in the body and is one of the most common tendon injuries in the adult population [1]. Management of chronic AT ruptures remains controversial due to potential surgical complications. Synthetic ligament has been an attractive alternative for reconstruction chronic AT tears. Long-term clinical results are lacking in the literature to confirm the safety and effectiveness of the LARS for AT reconstruction. Clinical research revealed a high percentage of complications in the long-term such as mechanical failures, foreign body synovitis, chronic effusions, and early arthritis [2]. This is a unique case report of long-term complication of AT reconstruction using LARS ligament and management by excision and reconstruction using Flexor Hallucis longus tendon.
Case Report
69-year-old male referred to foot and ankle clinic with gradually worsening lump on the back of ankle. The swelling had increased over a period of 18 months with associated pain and difficulty wearing footwear. He had Achilles tendon reconstruction using synthetic LARS ligament, 10 years ago after AT rupture. His past medical history includes Psoriasis and left bundle branch block. Clinically he had lobulated swelling in distal calf and posterior to ankle with no inflammatory skin changes or discharge to suggest an infection (Figure 1). MRI scan showed heterogeneous 16 × 6 cm collection within the Achilles tendon (Figure 2).

Figure 1: Picture of foot showing lobulated swelling over right Achilles tendon.
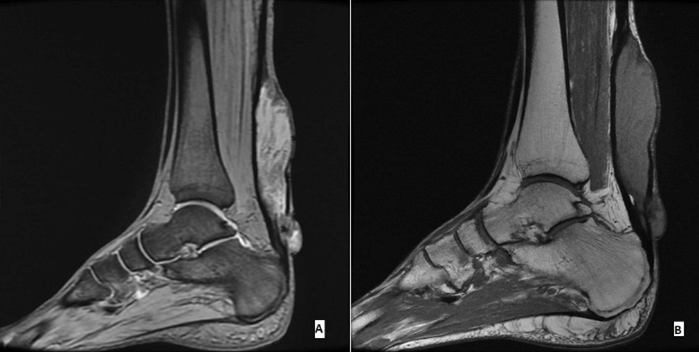
Figure 2: A) T2 and B) T1 sagittal MR images showing distinct heterogeneous mass in distal Achilles tendon.
Surgical Technique
With the patient prone, under general anaesthesia and thigh tourniquet control, an incision was made over previous scar over the palpable swelling at the site of Achilles tendon. On incising the swelling intact LARS ligament was identified which was successfully excised completely (Figure 3). Excised specimen was sent for histopathology which showed foreign body granuloma with no evidence of neoplasia or infection. We then reconstructed his Achilles tendon using a Flexor Halluces Longus (FHL) transfer. The patient recovered well from his surgery with no current complications.
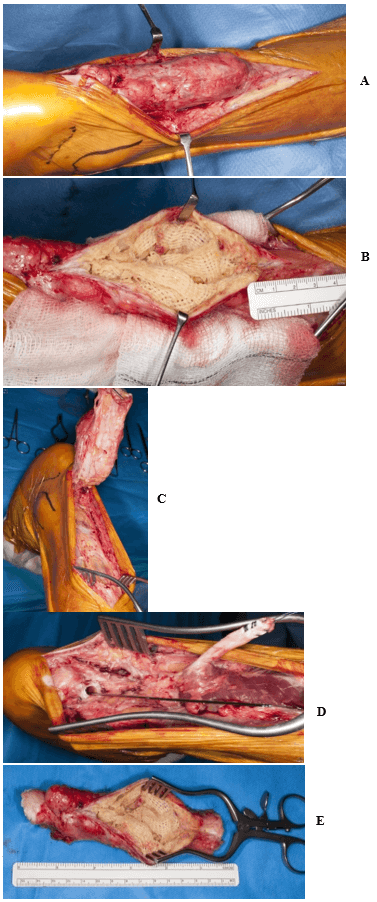
Figure 3: Demonstration of steps involved in surgical procedure. A) Intraoperative image of large cystic swelling over Achilles tendon. B) Synthetic LARS ligament found in the swelling on incising. C) Whole swelling was lifted off and excised. D) Intraoperative image showing FHL tendon lifted. E) Specimen of mass after excision.
Discussion
Synthetic materials were common in the 1980s as an alternative to biologic and allografts for different tendon ruptures to reduce donor site morbidity and eliminate the potential for disease transmission [2, 3]. One of these synthetic ligaments is the Ligament Advanced Reinforcement System (LARS) which was developed by J. P. Laboureau and was originally designed for PCL reconstruction but later on different clinical indications made it a common option for ACL and PCL reconstruction and shoulder repairs [3-6, 9]. The LARS ligament is a non-absorbable synthetic ligament device made of longitudinally arranged fibers of industrial strength synthetic terephthalic polyethylene polyester [5].
LARS ligament is commonly used for ACL, PCL, patellar tendon and ACJ stabilization with good surgical and clinical outcome [2, 3, 9]. There are few papers in literature where LARS ligament has been used for chronic AT ruptures [8]. Dhillon et al. demonstrated its use in a bilateral AT rupture with good functional outcome but was complicated by significant wound healing problems [10]. Literature has also shown successful medium-term results of using LARS ligament for chronic AT ruptures [8]. Clinical results in the long-term are lacking in the literature to confirm the safety and effectiveness of the LARS ligament [2]. One study has recommended not to use LARS ligament as a primary graft for ACL reconstruction [2]. A PubMed search revealed that there is only one case report about foreign body reaction with granuloma following AT reconstruction with LARS ligament [7].
Synthetic grafts, although an attractive option for orthopaedic surgeons due to the lack of donor side morbidity and easy availability, come with complications [2]. Being synthetic they are not truly bio compatible and present with long term complications like mechanical failures, foreign body synovitis, chronic effusions and early arthritis [11]. Patient in our study has a unique 10-year complication after LARS ligament reconstruction which was found intact on exploration with aggressive and symptomatic formation of foreign body granuloma.
Conclusion
There are no high-quality controlled studies in literature which determine the long-term complications of LARS ligament reconstruction. This case report certainly gives an idea of diagnosis and late complications after AT reconstruction using LARS ligament. We have also successfully demonstrated that en bloc resection and reconstruction with Flexor Hallucis Longus transfer is an effective salvage procedure.
Funding
None.
Conflicts of Interest
None.
Author Contributions
Noman Shakeel Niazi: Treating surgeon, conception and design, acquisition and interpretation of data, drafting and revising the article; Ahmed Aljawadi: Drafting and revising the article; Munir Khan: Acquisition and interpretation of data, drafting and revising the article; Anand Pillai: Treating surgeon, acquisition and interpretation of data and revising the article.
Article Info
Article Type
Case ReportPublication history
Received: Fri 12, Nov 2021Accepted: Sat 15, Jan 2022
Published: Thu 03, Feb 2022
Copyright
© 2023 Noman Shakeel Niazi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.RGM.2021.02.04
Figures & Tables
References
1. Lemme NJ, Li NY,
DeFroda SF, Kleiner J, Owens BD (2018) Epidemiology of Achilles Tendon Ruptures
in the United States: Athletic and Nonathletic Injuries From 2012 to 2016. Orthop
J Sport Med 6: 2325967118808238. [Crossref]
2. Tiefenboeck
TM, Thurmaier E, Tiefenboeck MM, Ostermann RC, Joestl J et al. (2015) Clinical and
functional outcome after anterior cruciate ligament reconstruction
using the LARS™ system at a minimum follow-up of 10 years. Knee 22:
565-568. [Crossref]
3. Machotka Z,
Scarborough I, Duncan W, Kumar S, Perraton L (2010) Anterior cruciate ligament
repair with LARS (ligament advanced reinforcement system): a systematic review.
Sports Med Arthrosc Rehabil Ther Technol 2: 29. [Crossref]
4. Mulford JS, Chen D
(2011) Anterior cruciate ligament reconstruction: A systematic review of
polyethylene terephthalate grafts. ANZ J Surg 81: 785-789. [Crossref]
5. Trieb K, Blahovec
H, Brand G, Sabeti M, Dominkus M et al. (2004) In vivo and in vitro cellular
ingrowth into a new generation of artificial ligaments. Eur Surg Res 36:
148-151. [Crossref]
6. Jia Z, Xue C, Wang
W, Liu T, Huang X et al. (2017) Clinical outcomes of anterior cruciate ligament
reconstruction using LARS artificial graft with an at least 7-year follow-up. Medicine
(Baltimore) 96: e6568. [Crossref]
7. Henry J, Konarski
AJ, Joseph L, Pillai A (2018) Foreign body reaction with granuloma following
Achilles tendon reconstruction with the LARS ligament. J Surg Case Rep
2018: rjx258. [Crossref]
8. Ibrahim SAR (2009)
Surgical Treatment of Chronic Achilles Tendon Rupture. J Foot Ankle Surg
48: 340-346. [Crossref]
9. Hunte TJAr, Abdus
Samee M, Balasubramanian S, Grocott N, McClelland D (2020). Medium-
to long-term results of acromioclavicular joint stabilisation using the
Ligament Augmentation Reconstruction System (LARS) ligament. Shoulder Elbow 12: 163-169. [Crossref]
10. Dhillon M, Chauhan D, Kumar V, Saini U (2010) Reconstruction of bilateral spontaneous chronic idiopathic Achilles tendon rupture using LARS ligament: Case report. Foot 20: 154-157. [Crossref]
11. Olson EJ, Kang JD, Fu FH, Georgescu HI, Mason GC et al. (1988) The biochemical and histological effects of artificial ligament wear particles: in vitro and in vivo studies. Am J Sports Med 16: 558-570. [Crossref]