Function Sparing Conservative Approach of a Low-Grade Chondrosarcoma of the Larynx: Case Report and Literature Review
A B S T R A C T
Background: Laryngeal cancer is relatively uncommon in Ecuador. Usually epithelial in origin, the most frequent histological type is squamous cell carcinoma. The most common mesenchymal tumor is chondrosarcoma. Most laryngeal chondrosarcomas are treated with total laryngectomy, but a conservative function sparing resection is recommended in low-grade limited tumors.
Case Report: In a 68-year-old female nonsmoker patient, a small tumor was found in the posterior left aspect of the cricoid cartilage in a computed tomography (CT) performed immediately after an unexpected difficulty to pass the endotracheal tube for a thoracoscopic biopsy of 4 cm tumor of the left lung, in another hospital. The patient underwent, then, an initial tracheostomy, a total thyroidectomy for a goiter and a biopsy of the tumor of the cricoid cartilage whose pathological study was inconclusive. One month later, a low-grade neuroendocrine pulmonary tumor was completed resected. Two years later, a CT scan showed the cricoid lesion with the same characteristics. At endoscopic video laryngoscopy, two subglottic masses that narrowed the airway in approximately 60% of the normal caliber, were observed located at the posterior and left walls. An intraluminal resection was performed through a transcricoid anterior approach. The pathological diagnosis was a low-grade chondrosarcoma. Tracheal decannulation was performed one month later. At an endoscopic video laryngoscopy performed six months post-operatively, the tracheal caliber and mucosa were normal. The patient remained with normal voice and breathing.
Conclusion: We report the second case of chondrosarcoma of the larynx in our country, treated by a conservative approach.
Keywords
Larynx, Larynx, Chondrosarcoma, Conservatory, Surgery
Introduction
Chondrosarcomas are tumors that include a wide spectrum of clinical and pathological findings, whose most frequent characteristic is the production of neoplastic cartilage. They account around 20% of all malignant bone tumors, and are the third most frequent malignant bone tumors. Between 2 and 5% are located in the head and neck region, mainly in the upper jaw [1]. A chondrosarcoma of the larynx was first described by Travers in 1816 but the term chondrosarcoma was introduced in 1935 by New [2]. It is the most common mesenchymal tumor of the larynx, although it only occurs between 0.5 and 1 % of tumors in this organ [1, 3]. Most publications have been about case reports, series have been rather scarce, and two reviews, Alvarez´s of 381 cases, and Chin´s of 592 cases, have been recently published [4, 5].
The incidence of laryngeal cancer in Ecuador is 1.3/100,000 in men and 0.3/100,000 in women, according to the National Tumor Registry of Ecuador [6]. No cases of chondrosarcoma of the larynx have been registered in this registry before 2015. Since then, we reported previously a case in a male patient treated with total laryngectomy and this is a second case of female patient that was treated by a function-conserving approach [7].
Case Report
In a 68-year-old female nonsmoker patient, who presented a long-standing moderate asymptomatic grade 3 goiter, a well-defined 4 cm tumor was diagnosed in the left lung at another hospital. A thoracoscopic biopsy planned under general anaesthesia, was not carried out because of an unexpected difficulty to pass the endotracheal tube. A computed tomography (CT) scan revealed a small tumor located in the posterior left aspect of the cricoid cartilage. The patient underwent, then, an initial tracheostomy, a total thyroidectomy and a cricoid lesion biopsy through the tracheostomy orifice. The pathological study confirmed the goiter but was inconclusive, with only cartilaginous tissue, for the cricoid lesion. One month later, the pulmonary tumor was resected and the histological study showed a low-grade neuroendocrine tumor completed resected. We evaluated the patient two years later, because of the pandemic. A new CT scan showed a lesion that arose from the posterior lamina of the cricoid cartilage, with the same size as previously, and characterized as a soft tissue, hypoattenuating mass, with lobulated margins, and stippled and coarse calcifications, with mild endolaryngeal extension. The lesion caused asymmetry of the pyriform sinuses, being smaller the left one (Figure 1).
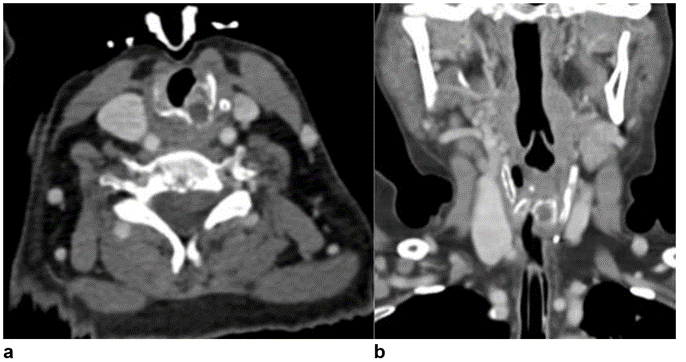
Figure 1: a) Axial and b) coronal contrast enhanced CT image shows a non-enhancing mass, that arises from the left posterior lamina of the cricoid cartilage with mild endolaryngeal extension causing asymmetry at the pyriform sinuses and mild airway narrowing.
At endoscopic video laryngoscopy, we observed two subglottic masses that narrowed the airway in approximately 60%: the larger one, smooth and rounded, was located at the posterior and left walls, and the second one, smaller and with similar characteristics, was located ahead; a notch separated them (Figure 2). An intraluminal resection was performed through a transcricoid anterior approach (Figures 3 & 4). A montgomery t-tube that was placed to prevent tracheal stenosis, had to be removed three days later because of obstruction due to a long clot. A tracheostomy tube left in place. Los cortes histológicos revelaron mostraron una mucosa erosionada por un infiltrado linfoplasmocitario intersticial en continuidad con cartílago hialino con gran celularidad y presencia de hipercromasia nuclear, atipia citológica leve, binucleación. multinucleación y varios focos de osificación. No se observó actividad mitótica ni necrosis. Se observó, adicionalmente, cartílago hialino de menor celularidad. The pathological diagnosis was a low-grade chondrosarcoma (Figure 5). Patient breathing and voice were satisfactory when the tracheostomy was left capped. An endoscopic exploration and a mild dilatation were performed three weeks later. Endotracheal lumen was satisfactory (Figure 6). Tracheal decannulation was performed one month later. At an endoscopic video laryngoscopy performed six months post-operatively, the tracheal caliber and mucosa were normal. The patient remained with normal voice and breathing.
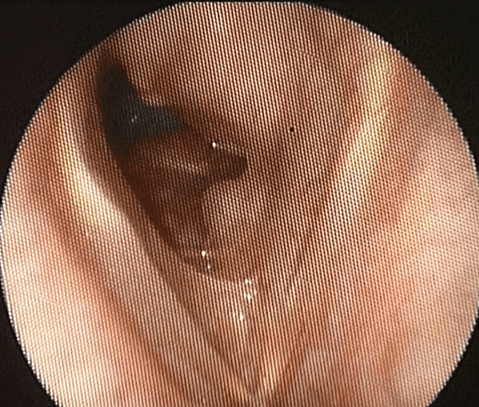
Figure 2: Endoscopic view of the mass located in the posterior left aspect of the subglottis.

Figure 3: View of the tumor through an anterior cricoid approach.

Figure 4: Surgical cavity after resection.

Figure 5: Matriz cartilaginosa con agrupaciones de condrocitos de distribución predominantemente difusa y en menor medida lobular, a mayor aumento observamos pleomorfismo celular de leve a moderado sin encontrarse actividad mitótica ni necrosis.

Figure 6: Endoscopic view one month after surgery.
Discussion
Chondrosarcoma originates in the hyaline cartilage, without evidence of elastic tissue, of the larynx, affecting the cricoid cartilage in 56 to 80% of cases, the thyroid cartilage in 11 to 20%, the arytenoids in 2 to 5 % and the epiglottis and the accessory cartilages in 1.5 3% [1, 4, 5]. No direct relationship has been found with the use of tobacco or alcohol consumption [1]. Mean age was 61 years and 62.5 years, and male gender in 74% and 60%, according to Alvarez´s review and Chin’s, respectively [4, 5]. Men: women´s ratio is 3.6:1 [1, 8, 9]. Peak age of presentation of this tumor coincides with the moment when the ossification of the cricoid cartilage is greater; and it is precisely in its posterior layer where this ossification occurs, and also, where the highest frequency of chondrosarcomas is found [1, 8].
Dyspnea, hoarseness and neck mass have been found to be the main symptoms [1, 4, 5]. Dyspnea seems to be related to an increase of the size of the tumor [9]. The presence of a cervical mass, and other symptoms, such as stridor, dysphagia, cough, seems to be related to the location and speed of growth of the tumor [1]. Impairment of movement of at least one vocal cord has been described in 17% of patients [4]. Our patient did not present dyspnea, had a good quality voice, and her grade 3 goiter was asymptomatic. The clinical picture in the majority of patients is indolent and of long duration, with an average of two years [10].
Imaging methods help to identify lesions suggesting chondroid neoplasm, including their morphological characteristics, location, dimensions, limits, and relation with adjacent structures. At CT, a chondrosarcoma appears as a lobulated mass, which usually arises from the posterior lamina of the cricoid cartilage, hypoattenuating in relation to muscle, and with coarse or stippled calcifications [11]. At MRI, it appears hyperintense at T2-weighted sequence and hypointense at T1 weighted sequence, representing the content of hyaline cartilage matrix. Some authors suggest that this imaging study is better because of its superior contrast resolution [10, 11]. Imaging studies do not allow to differentiate chondromas from chondrosarcomas, since most of them are low-grade, histologically [12]. In a recent meta-analysis, FDG PET showed excellent ability to diagnose chondrosarcoma, but restricted ability to differentiate benign cartilaginous lesions and G1 chondrosarcoma, but it could differentiate intermediate/high-grade chondrosarcoma from low-grade ones [13]. The CT scan of our patient showed characteristics consistent with chondrogenic tumor.
Grossly, they show a lobular and shiny "crunchy" consistency with a bluish-grey, semi-translucent colour and myxoid-mucinous material. Microscopically, they have a high nucleus/cytoplasm ratio with the presence of hyperchromatic nuclei [1]. Evans, in 1977, reported 3 degrees of differentiation of these tumors: low or grade1, intermediate or grade 2 and high or grade 3 [14]. Sixty-eight per cent to 80% of chondrosarcomas of the larynx are low-grade, have a less aggressive behaviour and may be difficult to differentiate from chondromas [1, 4, 5, 15]. Low to moderate grade lesions frequently associated with chondromas. (T1). Clinical suspicion and imaging studies should lead to a histological diagnosis of certainty by endoscopic biopsy. On laryngoscopy, the tumor usually appears as a smooth-surfaced, round, submucosal and hard consistency mass that is located in the subglottic region as in our patient [1]. As it is a submucosal lesion, sometimes this endoscopic biopsy may not be conclusive, as in the present case, and an open biopsy should be attempted. The study of the surgical piece provides the definitive histology, degree of differentiation, local extension and surgical margins [3].
The classic treatment of chondrosarcomas of the larynx is radical surgery with negative margins. Since in 75% to 80% of cases, chondrosarcomas of the larynx develop in the cricoid cartilage that maintains the lumen of the organ, if laryngeal function cannot be preserved, a total laryngectomy must be performed [16]. Partial surgery with preservation of function is recommended when the extent of the tumor and the patient's conditions allow it [1, 3, 15]. Zeitels recently reported 25 cases of posterior cricoid chondrosarcomas, mostly grade I-II, in whom some tumor was left in 23 of them, to preserve the cricoarytenoid -joint function. An ultra-function-sparing transcervical or transoral-endoscopic resection was performed in 20 of them, and no disease-specific deaths were observed after an 8-year median follow up [17]. Total cricoidectomy is an exceptional procedure that preserves laryngeal function and is indicated for low-grade and even intermediate-grade tumors [18]. Low morbidity, good quality of life, and good oncological control have been described with organ preservation surgery [19]. Total laryngectomy is recommended when the tumor affects more than 50% of the cricoid cartilage [10]. According to Alvarez´s review, total laryngectomy was performed in 34% of cases, tumor excision in 27%, partial laryngectomy in 24%, laser surgery in 9% and radiotherapy (RT) in 2% [4]. And according to Chin’s review, local excision was performed in 30% of cases, total laryngectomy in 29%, partial laryngectomy in 15%, endoscopic or microlaryngoscopic excision in 5%, laser excision in 4%, radiotherapy in 0.8% and chemotherapy in 0.2% [5].
Endoscopic treatment is indicated in case of small lesions. In this context, the use of laser therapy allows adequate control of bleeding [16]. Postoperative complications such as cervical emphysema, aspiration pneumonia, and others, have been reported in 1.3% of cases [5]. This tumor is characterized by being very little radiosensitive, so the use of radiotherapy (RT) as the first treatment continues to be controversial [15]. Its use is reserved, as complementary postoperative treatment, in high-grade tumors or tumors with compromised surgical margins. In addition, it can be indicated for inoperable patients or recurrences that cannot be adequately resected [15]. Postoperative RT was not considered in our patient.
As chondrosarcoma has a low potential for metastasis, adjuvant chemotherapy is not usually considered a treatment option [15]. Recurrence rates vary from 16 to 40% [1, 4, 5]. Long-term prognosis is good: 98%, 91%, 82% and 68% at 1, 5, 10 and 20 years, respectively [5]. Mean survival was 207 months, in Alvarez´s review, and it was affected by histological differentiation and type of surgery (lower survival for total laryngectomy compared to laser) [4]. Location of the tumor, histological grade and therapeutic approach was not related to survival, according to Chin’s review [5]. The development of metastases occurs in 2-8.5% of cases and are generally located in the lungs and bones [1, 3, 4].
In conclusion, our patient would be the second case of laryngeal chondrosarcoma reported in Ecuador according to the National Tumor Registry. Due to the slow clinical evolution of the tumor, a relatively limited extent within the cricoid cartilage on imaging studies, and a low-grade type of tumor, a function sparing approach was considered appropriate in this case.
Funding
None.
Article Info
Article Type
Case Report and Review of the LiteraturePublication history
Received: Wed 07, Feb 2024Accepted: Mon 26, Feb 2024
Published: Fri 29, Mar 2024
Copyright
© 2023 Luis Pacheco-Ojeda. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2024.01.04
Figures & Tables
References
1. Thompson LDR,
Gannon FH (2002) Chondrosarcoma of the larynx: a clinicopathologic study of 111
cases with a review of the literature. Am J Surg Pathol 26: 836-851. [Crossref]
2.
New
GB (1935) Sarcoma of the larynx: report of two cases. Arch Otolaryngol 21 .648-652.
3.
dos Santos Oliveira
JF, Pinto Lopes Branquinho FA, Tomé Nobre Monteiro AR, Correia Castro ME,
Ferreira Silva Guimarães AM (2014) Laryngeal chondrosarcoma - Ten years of
experience. Braz J Otorhinolaryngol 80: 354-358. [Crossref]
4. Álvarez Calderón-Iglesias O, Pérez Sayáns M, Hurtado
Ruzza R, Lorenzo Pouso A, Chamorro Petronacci C (2022) Survival outcomes in
laryngeal chondrosarcoma: a systematic review. Acta
Otorhinolaryngol Ital
42: 502-515. [Crossref]
5. Chin OY, Dubal PM,
Sheikh AB, Unsal AA, Woo Park RC (2017) Laryngeal chondrosarcoma: A systematic
review of 592 cases. Laryngoscope 127: 430-439. [Crossref]
6. Cueva P, Tarupi W,
Caballero H (2022) Cancer incidence and mortality in Quito: information to
monitor cancer control policies. Colomb Méd (Cali) 53: e2024929. [Crossref]
7.
Pacheco OL, Pontón
VP, Borja HT, Ayala OA (2017) Condrosarcoma de la laringe: reporte de un caso y
revisión de la literatura. Rev Otorrinolaringol Cir Cabeza Cuello 77:
175-180.
8. Thomé R, Thomé DC,
de la Cortina RA (2001) Long-term follow-up of cartilaginous tumours of the
larynx. Otolaryngol Head Neck Surg 124: 634-640. [Crossref]
9. Dubal P, Svider PF,
Kanumuri VV, Patel AA, Baredes S et al. (2014) Laryngeal Chondrosarcoma: A
Population-Based Analysis. Laryngoscope 124: 1877-1881. [Crossref]
10. Wang Q, Chen H,
Zhou S (2015) Chondrosarcoma of the larynx: report of two cases and review of
the literature. Int J Clin Exp Pathol 8: 2068-2073. [Crossref]
11. Ong AC, Huh EH,
Moreland AJ, Rooper LM, Aygun N et al. (2020). Nonepithelial tumors of the larynx:
Single-institution 13-year review with radiologic-pathologic correlation. Radiographics
40: 2011-2028. [Crossref]
12. Bathala S, Berry S,
Evans RA, Brodie S, Altaan O (2008) Chondrosarcoma of larynx: review of
literature and clinical experience. J Laryngol Otol 122: 1127-1129. [Crossref]
13. Zhang Q, Xi Y, Li
D, Yuan Z, Dong J (2020) The utility of 18F-FDG PET and PET/CT in
the diagnosis and staging of chondrosarcoma: a meta-analysis. J Orthop Surg Res 15: 229. [Crossref]
14. Evans HL, Ayala AG,
Romsdahl MM (1977) Prognostic Factors in Chondrosarcoma of bone. A
clinicopathologic analysis with emphasis on histologic grading. Cancer
40: 818-831. [Crossref]
15. Buda I, Hod R,
Feinmesser R, Shvero J (2012) Chondrosarcoma of the Larynx. Isr Med Assoc J
14: 681-684. [Crossref]
16. Sauter A, Bersch C,
Lambert KL, Hörmann K, Naim R (2007) Chondrosarcoma of the larynx and review of
the literature. Anticancer Res 27: 2925-2929. [Crossref]
17. Zeitels SM, Baird
BJ (2022) Surgical Treatment Strategies for Laryngeal Chondrosarcomas: A Single
Institution Investigation. Laryngoscope 132: 169-176. [Crossref]
18. de Vincentiis M, Greco A, Fusconi M, Pagliuca G, Martellucci S et al. (2011) Total cricoidectomy in the treatment of laryngeal chondrosarcomas. Laryngoscope 121: 2375-2380. [Crossref]
19. Piazza C, Del Bon F, Grazioli P, Mangili S, Barbieri D et al. (2014) Organ preservation surgery for low- and intermediate-grade laryngeal chondrosarcomas: analysis of 16 cases. Laryngoscope 124: 907-912. [Crossref]