HE4 in Various Body Fluids: A Prospective Pilot Study
A B S T R A C T
Introduction: Human epididymis protein 4 (HE4) is a glycoprotein that is a sensitive and specific serum biomarker for patients with suspected ovarian cancer. HE4 is also secreted in different body fluids such as cervical mucus or urine, which could provide an easy alternative for screening purposes. HE4 protein secretion in different body fluids was analysed in 11 healthy controls and in 10 patients with a benign, 10 with a borderline and 22 with a malignant ovarian tumor.
Materials and Methods: Preoperative samples of serum, urine, cervical mucus, saliva, and ascites were collected to measure HE4 with an ELISA assay. Urinary creatinine concentration and cervical total protein concentrations were used as reference analytes, and ratios with HE4 were calculated.
Results: Median HE4 concentration in urine was higher in patients with epithelial ovarian cancer (EOC) compared to healthy controls and patients with a benign or borderline mass (p=0.02). HE4/creatinine ratio could differentiate healthy controls from EOC and benign ovarian disease from EOC (AUC 0.76, 95% CI 0.58-0.94 and AUC 0.71, 95% 0.52-0.89, respectively). HE4 in ascites was significantly higher in patients with EOC or borderline ovarian mass compared to patients with a benign ovarian mass (p=0.04). HE4 concentrations in cervical mucus and saliva were not significantly higher in patients with EOC.
Conclusion: This study shows that HE4 is abundant in body fluids other than blood and suggests that urinary HE4 levels can be used as a non-invasive diagnostic alternative to detect EOC.
Keywords
HE4, body fluids, ovarian cancer, urine, tumor marker
Introduction
Biomarkers are routinely used in screening, diagnosis, monitoring treatment, follow-up, and prognosis of (malignant) diseases. Although biomarkers are often measured in serum, other body fluids could potentially also be used for this purpose. The advantage of other (often easy obtainable) fluids is that they can be used in a primary care setting where venipuncture facilities are not available. Human epididymis protein 4 (HE4) is a relatively new serum biomarker used in the diagnosis of EOC with a sensitivity comparable to CA125 but with higher specificity [1]. HE4 is a member of the whey-acid four-disulfide core (WFDC) protein family that comprises a heterogeneous group of small acid-stable and heat-stable proteins with different biological functions. HE4 is also known as WFDC2 and the gene coding for HE4 is located on chromosome 20q13 [2]. Although the function of the HE4 protein remains largely unknown, it is becoming clearer that HE4 is frequently amplified in EOC, while its expression in normal tissues, including the ovary, is relatively low [3, 4]. Among normal tissue, the highest expression is found in the glandular epithelium of the respiratory and genital tract [4-6]. HE4 protein has a small molecular weight (25kD), is secreted by the kidneys and can therefore be detected in urine [7, 8].
EOC cells express HE4 and secrete HE4 as an N-glycosylated protein in the extracellular environment [9]. This suggests that HE4 cannot only be detected in serum but also in swabs from other (easily accessible) body fluids like cervical or vaginal fluid. Also, HE4 protein might simply be transferred through the fallopian tubes and the uterine cavity to the cervix following the anatomical route. It is described that precursor lesions of high-grade serous ovarian carcinomas shed cells which can then be detected in cervical cytological smears [10, 11]. This probably precedes the onset of clinical symptoms caused by high grade EOC and the detection of transvaginal ultrasound [12, 13]. Whether HE4 secreted by EOC cells can also be detected in a cervical smear has not been evaluated before. Evaluation of the HE4 protein secretion in body fluids other than blood can determine the feasibility of a clinical trial using alternatives for serum HE4 measurement. Therefore, we performed a pilot study to evaluate the possibility of detecting HE4 in different body fluids of healthy women, patients with benign or borderline ovarian lesion, and patients with EOC, and to evaluate which fluids are best used in further prospective research.
Methods
I Patient Recruitment and Sample Collection
Patients were included between April 2014 and October 2016. Samples of healthy women, patients with a benign or borderline ovarian mass, and patients with confirmed EOC were collected after informed consent was obtained. The controls were healthy women of different age at risk for developing EOC because of a genetic predisposition who were planned for risk-reducing salpingo-oophorectomy. They had no documented history of EOC and in none of them, an adnexal abnormality was seen on transvaginal ultrasound. An extra blood sample was collected and women were asked to donate a saliva and urine sample and the principal investigator took a cervical swab. Final pathology after risk-reducing salpingo-oophorectomy was checked to exclude (pre)malignancy.
In the other groups, women that were referred to our oncologic center for surgery because of an ovarian mass were included. In these patients, the malignant potential of the adnexal mass was not known before surgery; hence they were assigned to the definitive group (benign, borderline, or malignant) after the final pathology report. Also, samples from patients with known FIGO stage III EOC that underwent primary or interval cytoreductive surgery were collected as positive controls. In all of these patients, an extra blood sample was collected for the measurement of serum HE4, a saliva sample was collected the day before surgery, while the urine sample, cervical swab and ascites sample (if present) were collected preoperative before the incision while the patient was under general anaesthesia or during surgery.
II HE4 Measurement
The HE4 EIA is a solid-phase, non-competitive immunoassay based upon the direct sandwich technique using two mouse monoclonal antibodies, 2H5 and 3D8, directed against two epitopes in the C-WFDC domain of HE4. Samples are incubated together with biotinylated anti-HE4 monoclonal antibody (MAb) 2H5 in streptavidin-coated microstrips. HE4 present in calibrators or samples is absorbed to the streptavidin-coated microstrips by the biotinylated anti-HE4 MAb during the incubation. The strips are then washed and incubated with HRP labeled anti-HE4 MAb 3D8. After washing, buffered substrate/chromogen reagent (hydrogen peroxide and 3, 3’, 5, 5’ tetra-methyl-benzidine) is added to each well and the enzyme reaction is allowed to proceed. During the enzyme reaction, a blue colour will develop if antigen is present. The intensity of the colour is proportionate to the amount of HE4 present in the samples. The colour intensity is determined in a microplate spectrophotometer at 620 nm (or optionally at 405 nm after the addition of stop solution). Calibration curves are constructed for each assay by plotting absorbance value versus the concentration for each calibrator. The HE4 values of patient samples are then read from the calibration curve. HE4 values in serum are presented in pmol/L while values in other body fluids are presented in nmol/L.
Since no 24-hour urine was collected, urinary creatinine concentration (mmol/L) was determined as a quality assurance tool to assess the accuracy of a 24-hour secretion. Comprehensive proteomic analysis of cervical and vaginal fluid showed a relative abundance of serum protein albumin [14]. Therefore, total protein (g/L) were determined in cervical fluid and used as a reference analyte.
III Statistical Analysis
A power calculation was not performed because of the hypothesis-generating aspect of this study. Moreover, the concentration in other body fluids is largely unknown, so to estimate the aimed difference is impossible. Creatinine in urine and protein in the cervical fluid was used as reference analytes and we calculated the ratio HE4/creatinine in urine and HE4/total protein in cervical fluid. Median HE4 concentrations in serum and calculated ratios for all groups were presented in boxplot graphs. Kruskal-Wallis test was used to determine a statistically significant difference between median HE4 concentrations between groups. Receiver operating characteristics (ROC) curves were computed to illustrate the discriminative potential of each marker between healthy controls and patients with EOC. The area under the curve (AUC) was calculated with corresponding 95% confidence intervals. The ROC analysis was also used to determine a cut-off value for each marker that yields high sensitivity. A p-value <0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics version 22.
Results
A total of 245 samples of 53 patients were collected: 11 controls, 10 patients with a benign ovarian mass, 10 with a borderline ovarian mass and 22 with EOC. Patients and tumor characteristics are summarized in (Table 1). Mean age of patients was statistically significant between groups (p=0.006), with the highest age found in patients with EOC. The majority of the patients (n=15, 68%) with EOC were diagnosed with a serous type adenocarcinoma, followed by mucinous adenocarcinoma (n=3, 14%) and carcinosarcoma (n=2, 9%). The FIGO stage (low versus high) was equally divided between groups. HE4 was detectable in all tested body fluids and the concentration was higher in urine, cervical fluid, saliva and ascites compared to the concentration measured in serum (Table 2).
Median HE4 concentrations per group are summarized in (Table 2) and presented in (Figure 1). In serum and urine, the highest HE4 concentrations were measured in patients with EOC (p<0.001 and p=0.02, respectively). The HE4/creatinine ratio showed significantly higher values in patients with EOC compared to other groups (p=0.02). HE4/creatinine ratio was higher in patients with advanced-stage (FIGO III-IV) EOC compared to those with early- stage (FIGO I-II) EOC (3.72 versus 0.78 respectively, p=0.05). The highest cervical HE4 concentration was measured in a patient with a borderline ovarian mass, but no statistic significant difference was found in the cervical HE4/protein ratio between groups (p=0.79). HE4 concentration in ascites was significantly higher in patients with a borderline or malignant ovarian mass compared to patients with a benign ovarian mass. No significant difference was measured in median HE4 concentration in saliva between groups.
Table 1: Patients and tumor characteristics.
|
|
Control n=11 (%) |
Benign n=10 (%) |
Borderline n=10 (%) |
Malignant n=22 (%) |
|
Mean age in years (SD) |
48 (8.3) |
58 (8.8) |
51 (16.8) |
64 (12.8) |
|
Menopausal state Premenopausal Postmenopausal |
7 (64%) 4 (36%) |
4 (40%) 6 (60%) |
5 (40%) 5 (50%) |
3 (14%) 19 (86%) |
|
Benign histology Serous cystadenoma Mucinous cystadenoma Adenofibroma Other |
NA
|
4 (40%) 3 (30%) 2 (20%) 1 (10%) |
NA |
NA |
|
Borderline histology Serous borderline Mucinous borderline |
NA
|
NA |
6 (60%) 4 (40%) |
NA |
|
Malignant histology Serous adenocarcinoma Mucinous adenocarcinoma Endometrioid adenocarcinoma Clear cell carcinoma Carcinosarcoma |
NA
|
NA |
NA |
15 (68%) 3 (14%) 1 (4.5%) 1 (4.5%) 2 (9%) |
|
FIGO stage I-II III-IV |
NA |
NA |
NA |
11 (50%) 11 (50%) |
Abbreviations: SD; standard deviation, NA; not applicable.
Table 2: Median HE4 values (range) in different body fluids presented by group.
|
|
Control n=11 |
Benign n=10 |
Borderline n=10 |
Malignant n=22 |
Significancea |
|
Serum (pmol/L) |
42 (29-68) |
77 (38-154) |
81 (44-126) |
137 (46-3328) |
p<0.001 |
|
Urine (nmol/L) |
5.28 (0.70-18.7) |
6.79 (3.26-41.2) |
7.62# (1.94-17.0) |
20.2 (0.4-904) |
p=0.02 |
|
HE4/creatinine ratio |
0.72 (0.24-0.90) |
0.93 (0.27-1.33) |
1.03# (0.55-3.69) |
1.60 (0.11-35.1) |
p=0.02 |
|
Cervix (nmol/L) |
0.81 (0.28-9.67) |
6.99 (0.04-49.0) |
6.38# (0.14-35.7) |
5.81 (0.02-29.0) |
p=0.09 |
|
Cervical HE4/protein ratio (nmol/g) |
6.73 (0.87-44.2) |
12.0 (0.36-107) |
16.8# (0.36-261) |
5.77 (0.05-125.6) |
p=0.79 |
|
Saliva (nmol/L) |
15.2 (2.97-43.8) |
13.7 (6.37-56.5) |
27.1# (5.26-69.3) |
20.8 (6.55-78.8) |
p=0.45 |
|
Ascites (nmol/L) |
NA |
0.29 (0-1.76) |
0.91# (0.43-6.63) |
1.66 (0.02-13.4) |
p=0.04 |
a Statistical significant difference in median values between groups was calculated using Kruskal Wallis test; # missing values of two patients.
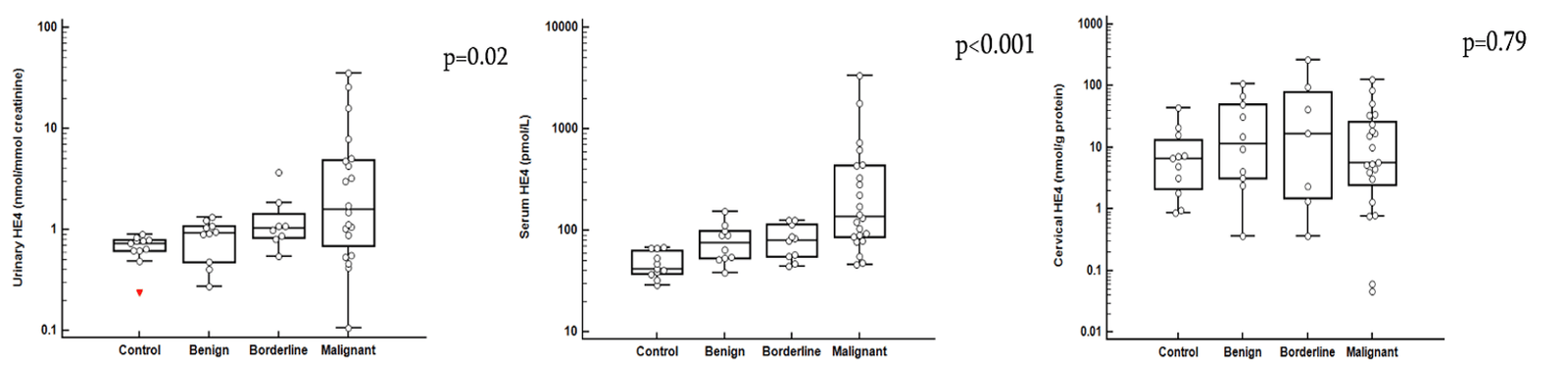
Figure 1: Boxplot graph illustrating the median serum HE4 concentration, HE4/creatinine ratio in urine and HE4/total protein ratio in cervical fluid.
ROC Analysis
ROC analysis of serum HE4, HE4/creatinine ratio and HE4/protein ratio were performed and are presented in (Figure 2). Serum HE4 shows the highest discriminative value in differentiating healthy controls from patients with EOC, followed by HE4/creatinine (AUC 0.96, 95% CI 0.89-1.00 and AUC 0.76, 95% CI 0.58-0.94 respectively) (Figure 2A). In (Figure 2B), ROC analysis in patients with benign ovarian disease and EOC is illustrated. Serum HE4 and HE4/creatinine ratio display a comparable AUC (AUC 0.76, 95% CI 0.58-0.93 and AUC 0.71, 95% CI 0.52-0.89). Sensitivities and corresponding cut-off values were calculated at a set specificity of 95%. For serum HE4, sensitivity was 89% with a corresponding value of 67 pmol/L. HE4/creatinine ratio had a sensitivity of 68% with a ratio of 0.89.
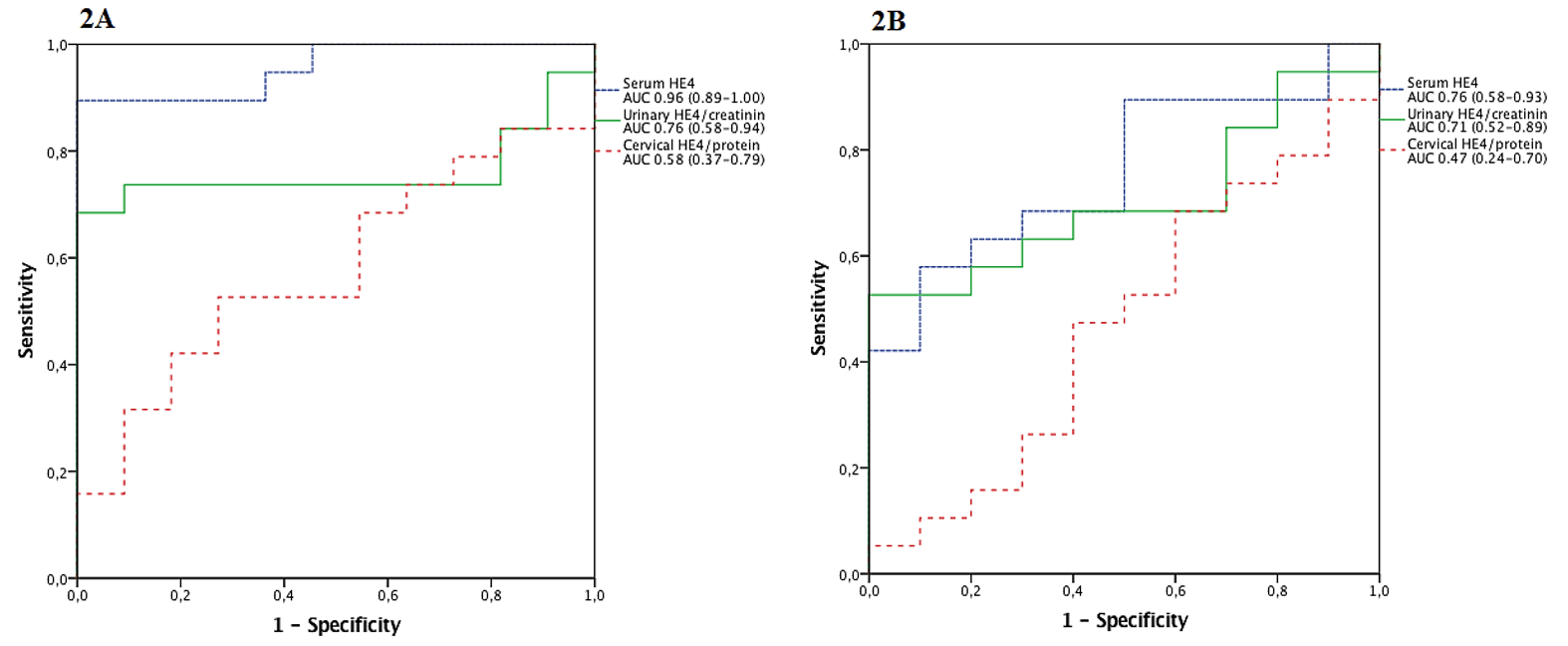
Figure 2: ROC curves with AUC and corresponding 95% CI illustrating the discriminative value A) between a healthy control group and EOC and B) patients with a benign ovarian mass and EOC.
Discussion
In this study, we showed that HE4 can not only be measured in serum but also in other body fluids such as urine, cervical mucus, saliva, and ascites. Higher HE4 concentrations were found in urine of patients with EOC compared to patients with a borderline or benign ovarian mass and healthy controls. This suggests that a urinary HE4 test might be worthwhile to investigate in a prospective trial for use in the diagnosis of patients with EOC. For the early diagnosis of patients with a malignant ovarian mass, a test that exhibits high sensitivity and specificity is needed. Serum CA125 is a sensitive marker to detect high stage EOC but is only elevated in 50% of patients with low stage EOC. Moreover, it lacks specificity. Serum biomarker HE4 has an advantage over serum CA125 because less false-positive test results are seen in patients with benign ovarian disease. As a consequence of the renal clearance of HE4, high urinary HE4 concentrations were measured in this study cohort. Our data show that urinary HE4/creatinine level has a high discriminative value that is comparable to serum HE4 with respect to the differentiation between patients with a benign ovarian mass and patients with EOC. These results are supported by the results of previous studies [7, 15].
From previous studies, we know that serum HE4 is correlated to age and this might partially have influenced our results concerning the serum HE4 concentrations [16, 17]. Because an impaired renal function is positively related to serum HE4 concentrations, measuring a HE4/creatinine ratio in urine is possibly a more reliable test in these patients [17, 18]. Preliminary data on a small cohort of patients indicated that HE4 is earlier detectable in urine than serum before the patient relapse [8]. Since there is often no curative treatment for recurrent ovarian cancer, the use of early detection hereof is debatable.
A cervical swab, as is routinely taken in cervical cancer screening, was theoretically an attractive alternative to screen for ovarian malignancy. We hypothesized that HE4 could be secreted by cells from (pre)cancerous lesions in the fallopian tubes and be transferred to the cervix and detectable by a cervical swab. However, the results of this study show that HE4 is also detected in the cervical mucus of healthy controls and did not show significant different concentrations compared to patients with advanced EOC. Moreover, no significant difference was found in HE4/total protein ratios between different groups. This does not support the future use of cervical HE4 measurements in screening or detection of early-stage EOC. Whether HE4 has a function in the natural vaginal composition is not fully understood yet, but the composition of the vaginal microbiota seems to influence the vaginal and cervical HE4 concentration [19, 20].
Previous studies have reported a high expression of HE4 in the respiratory tract also in a healthy population [6, 21]. In concordance, we found high HE4 concentrations in saliva in all patients including healthy controls. Therefore, HE4 in saliva cannot be used as a biomarker for the detection of EOC. Higher HE4 concentrations in ascites of patients with EOC are probably caused by the direct secretion of HE4 by malignant cells in the peritoneal fluid or on the peritoneum. Because ascites is present in high stage disease, ascites is not very useful as screening fluid. However, measurement of HE4 in ascites can be helpful to differentiate between EOC and ovarian metastases from other malignancies [22].
We were the first to analyse HE4 secretion in different body fluids, of which some have never been investigated before (cervical mucus, saliva, ascites) in the same cohort of patients. This study has a few limitations. First, we included a relatively small number of patients because this was a pilot study to investigate whether it was feasible to detect the HE4 antigen in other body fluids than serum. Despite this relatively small number of patients in this study, we do not expect different results concerning the HE4 secretion in saliva when more patients are included. Further studies should therefore focus on the HE4 secretion in urine and further elucidate the secretion in cervical mucus. Second, we found higher serum HE4 values in patients with benign disease compared to healthy controls, which was in contrast with our previous study [23]. This might be explained by the small number of patients included in this pilot study. However, in concordance with this study, HE4 values in patients with EOC were still significantly higher than of patients with benign or borderline ovarian disease [23]. In conclusion, we showed that HE4 is abundant in other body fluids than serum. Urinary HE4 concentration in combination with the urinary creatinine level is the most promising test option for future research to a new and simple non-invasive test in patients with an ovarian mass.
Conflicts of Interest
None.
Acknowledgements
The authors would like to thank Fujirebio Diagnostics Inc for partially funding this study. This work was in part supported by an unrestricted grant of HANARTH Foundation. The source of funding did not have any influence on the design of the study, collection, analysis and interpretation of the data and in writing the manuscript.
Funding
Fujirebio Diagnostics Inc partially funded research time of author A. Stiekema.
Article Info
Article Type
Research ArticlePublication history
Received: Fri 19, Jun 2020Accepted: Mon 09, Nov 2020
Published: Mon 30, Nov 2020
Copyright
© 2023 Anna Stiekema. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.COR.2020.11.06
Figures & Tables
Table 1: Patients and tumor characteristics.
|
|
Control n=11 (%) |
Benign n=10 (%) |
Borderline n=10 (%) |
Malignant n=22 (%) |
|
Mean age in years (SD) |
48 (8.3) |
58 (8.8) |
51 (16.8) |
64 (12.8) |
|
Menopausal state Premenopausal Postmenopausal |
7 (64%) 4 (36%) |
4 (40%) 6 (60%) |
5 (40%) 5 (50%) |
3 (14%) 19 (86%) |
|
Benign histology Serous cystadenoma Mucinous cystadenoma Adenofibroma Other |
NA
|
4 (40%) 3 (30%) 2 (20%) 1 (10%) |
NA |
NA |
|
Borderline histology Serous borderline Mucinous borderline |
NA
|
NA |
6 (60%) 4 (40%) |
NA |
|
Malignant histology Serous adenocarcinoma Mucinous adenocarcinoma Endometrioid adenocarcinoma Clear cell carcinoma Carcinosarcoma |
NA
|
NA |
NA |
15 (68%) 3 (14%) 1 (4.5%) 1 (4.5%) 2 (9%) |
|
FIGO stage I-II III-IV |
NA |
NA |
NA |
11 (50%) 11 (50%) |
Abbreviations: SD; standard deviation, NA; not applicable.
Table 2: Median HE4 values (range) in different body fluids presented by group.
|
|
Control n=11 |
Benign n=10 |
Borderline n=10 |
Malignant n=22 |
Significancea |
|
Serum (pmol/L) |
42 (29-68) |
77 (38-154) |
81 (44-126) |
137 (46-3328) |
p<0.001 |
|
Urine (nmol/L) |
5.28 (0.70-18.7) |
6.79 (3.26-41.2) |
7.62# (1.94-17.0) |
20.2 (0.4-904) |
p=0.02 |
|
HE4/creatinine ratio |
0.72 (0.24-0.90) |
0.93 (0.27-1.33) |
1.03# (0.55-3.69) |
1.60 (0.11-35.1) |
p=0.02 |
|
Cervix (nmol/L) |
0.81 (0.28-9.67) |
6.99 (0.04-49.0) |
6.38# (0.14-35.7) |
5.81 (0.02-29.0) |
p=0.09 |
|
Cervical HE4/protein ratio (nmol/g) |
6.73 (0.87-44.2) |
12.0 (0.36-107) |
16.8# (0.36-261) |
5.77 (0.05-125.6) |
p=0.79 |
|
Saliva (nmol/L) |
15.2 (2.97-43.8) |
13.7 (6.37-56.5) |
27.1# (5.26-69.3) |
20.8 (6.55-78.8) |
p=0.45 |
|
Ascites (nmol/L) |
NA |
0.29 (0-1.76) |
0.91# (0.43-6.63) |
1.66 (0.02-13.4) |
p=0.04 |
a Statistical significant difference in median values between groups was calculated using Kruskal Wallis test; # missing values of two patients.
References
- Moore RG, Brown AK, Miller MC, Skates S, Allard WJ et al. (2008) The use of multiple novel tumor biomarkers for the detection of ovarian carcinoma in patients with a pelvic mass. Gynecol Oncol 108: 402-408. [Crossref]
- Kirchhoff C, Habben I, Ivell R, Krull N (1991) A major human epididymis-specific cDNA encodes a protein with sequence homology to extracellular proteinase inhibitors. Biol Reprod 45: 350-357. [Crossref]
- Hellström I, Raycraft J, Hayden Ledbetter M, Ledbetter JA, Schummer M et al. (2003) The HE4 (WFDC2) protein is a biomarker for ovarian carcinoma. Cancer Res 63: 3695-3700. [Crossref]
- Hertlein L, Stieber P, Kirschenhofer A, Krocker K, Nagel D et al. (2012) Human epididymis protein 4 (HE4) in benign and malignant diseases. Clin Chem Lab Med 50: 2181-2188. [Crossref]
- Galgano MT, Hampton GM, Frierson HF (2006) Comprehensive analysis of HE4 expression in normal and malignant human tissues. Mod Pathol 19: 847-853. [Crossref]
- Bingle L, Singleton V, Bingle CD (2002) The putative ovarian tumour marker gene HE4 (WFDC2), is expressed in normal tissues and undergoes complex alternative splicing to yield multiple protein isoforms. Oncogene 21: 2768-2773. [Crossref]
- Hellstrom I, Heagerty PJ, Swisher EM, Liu P, Jaffar J et al. (2010) Detection of the HE4 protein in urine as a biomarker for ovarian neoplasms. Cancer Lett 296: 43-48. [Crossref]
- Liao JB, Yip YY, Swisher EM, Agnew K, Hellstrom KE et al. (2015) Detection of the HE4 protein in urine as a biomarker for ovarian neoplasms: Clinical correlates. Gynecol Oncol 137: 430-435. [Crossref]
- Drapkin R, Von Horsten HH, Lin Y, Mok SC, Crum CP et al. (2005) Human epididymis protein 4 (HE4) is a secreted glycoprotein that is overexpressed by serous and endometrioid ovarian carcinomas. Cancer Res 65: 2162-2169. [Crossref]
- Takeshima N, Hirai Y, Yamauchi K, Hasumi K (1997) Clinical usefulness of endometrial aspiration cytology and CA-125 in the detection of fallopian tube carcinoma. Acta Cytol 41: 1445-1450. [Crossref]
- Takeshina T, Ono M, Kanda Y, Sagae S, Hayakawa O et al. (1988) Cervicovaginal and endometrial cytology in ovarian cancer. Acta Cytol 32: 159-162. [Crossref]
- Weinberger V, Bednarikova M, Cibula D, Zikan M (2016) Serous tubal intraepithelial carcinoma (STIC)-clinical impact and management. Expert Rev Anticancer Ther 16: 1311-1321. [Crossref]
- Otsuka I, Kameda S, Hoshi K (2013) Early detection of ovarian and fallopian tube cancer by examination of cytological samples from the endometrial cavity. Br J Cancer 109: 603-609. [Crossref]
- Tang LJ, Seta FD, Odreman F, Venge P, Piva C et al. (2007) Proteomic Analysis of Human Cervical-Vaginal Fluids. J Proteome Res 6: 2874-2883. [Crossref]
- Macuks R, Baidekalna I, Donina S (2012) Urinary concentrations of human epidydimis secretory protein 4 (He4) in the diagnosis of ovarian cancer: a case-control study. Asian Pac J Cancer Prev 13: 4695-4698. [Crossref]
- Moore RG, Miller MC, Eklund EE, Lu KH, Bast RC et al. (2012) Serum levels of the ovarian cancer biomarker HE4 are decreased in pregnancy and increase with age. Am J Obstet Gynecol 206: 349. [Crossref]
- Bolstad N, Øijordsbakken M, Nustad K, Bjerner J (2012) Human epididymis protein 4 reference limits and natural variation in a Nordic reference population. Tumor Biol 33: 141-148. [Crossref]
- Nagy B, Krasznai ZT, Balla H, Csoban M, Antal Szalmás P et al. (2012) Elevated human epididymis protein 4 concentrations in chronic kidney disease. Ann Clin Biochem 49: 377-380. [Crossref]
- Orfanelli T, Jayaram A, Doulaveris G, Forney LJ, Ledger WJ et al. (2014) Human Epididymis Protein 4 and Secretory Leukocyte Protease Inhibitor in Vaginal Fluid: Relation to Vaginal Components and Bacterial Composition. Reprod Sci 21: 538-542. [Crossref]
- Grande G, Milardi D, Vincenzoni F, Pompa G, Biscione A et al. (2015) Proteomic characterization of the qualitative and quantitative differences in cervical mucus composition during the menstrual cycle. Mol Biosyst 11: 1717-1725. [Crossref]
- Bingle L, Cross SS, High AS, Wallace WA, Rassl D et al. (2006) WFDC2 (HE4): a potential role in the innate immunity of the oral cavity and respiratory tract and the development of adenocarcinomas of the lung. Respir Res 7: 61. [Crossref]
- Stiekema A, Van de Vijver KK, Boot H, Broeks A, Korse CM et al. (2017) Human Epididymis protein 4 immunostaining of malignant ascites differentiates cancer of Mullerian origin from gastrointestinal cancer. Cancer Cytopathol 125: 197-204. [Crossref]
- Stiekema A, Lok CAR, Kenter GG, van Driel WJ, Vincent AD et al. (2014) A predictive model combining Human Epididymis protein 4 and radiologic features for the diagnosis of ovarian cancer. Gynecol Oncol 132: 573-577. [Crossref]