Iatrogenic Abdominal Firm Lump: A Case Report of a Retained Surgical Item Detected 8 Years Post-Abdominoplasty
A B S T R A C T
Introduction and Importance: Retained surgical body (RSB) is unusual life-threatening condition occurred postoperatively. Despite its rarity, multiple protective and management policies were documented by policymakers.
Case Presentation: A 62-year-old female patient presented with a few months’ history of abdominal mass. She presented to our hospital 8 years post-abdominoplasty that was performed in a private sector. The underlying cause of the abdominal mass was identified by abdominal and pelvic computed tomography (CT) with IV contrast as a surgically retained foreign tubular object. Then, the decision was made to proceed with an open surgical technique to remove the RSB, which was defined as a missed drain tube. The postoperative period was uneventful.
Clinical Discussion: Post-operative RSB, as a retained drain fragment, is a surgical challenge that necessitates standardization of error reporting strategies, awareness enhancement, and improvement of professional communication between surgical teams in the operation room.
Conclusion: This case highlights the serious consequences of RSB and the radiologic tools in foreign materials identification. We report the case of a 62-year-old female patient with a long-standing history of abdominal mass, found to be caused by an unintentionally retained drain tube missed 8 years post-abdominoplasty.
Keywords
Retained surgical bodies, foreign bodies, seroma, abdominoplasty, retained drain, case report
Highlights
• The occurrence of foreign objects retention is unusual event, and its consequence is serious.
• Radiographic diagnostic tools are crucial for surgically retained materials identification.
• Surgical removal of the retained material, including laparotomy, is the main treatment approach.
• Policymakers have urged for the establishment of error reporting systems in order to gather knowledge on the patterns that explain particular kinds of errors.
Introduction
Retained surgical body (RSB) is a life-threatening situation that carries a risk of surgical reoperation [1]. In the literature, multiple retained items were detected including sponges, sharps, instruments, small objects, and device fragments [2]. These retained objects are usually detected in body cavities and confirmed by computed tomography (CT) [3]. The incidence of cases of surgical material retained in the abdominal cavity is low, accounting for between 0.3 to 1.0 cases of intra-abdominal surgical interventions [4, 5]. Significant complications that arise from RSIs include repeated hospitalization, necessitating an additional surgical procedure to repair the injury, sepsis or infection, fistula or small bowel obstruction, and visceral perforation [5].
Here we highlight a 62-year-old female patient who presented with a few months’ history of a painless abdominal lump found to be due to unintentionally retained drain from 8 years of abdominoplasty. Our work has been reported in line with the SCARE Guidelines 2020 criteria [6].
Case Presentation
A 62-year-old female patient presented with a few months’ history of a painless abdominal lump. This abdominal mass was first noticed 8 years ago following abdominoplasty in a private hospital. The mass/lump is located near the surgical incision and extends up. It has been neglected since that time due to its smaller size, but the recent increase in size that was resulted in the development of discomfort symptoms, especially those associated with movement. On admission, laboratory investigations were unremarkable. The physical examination revealed a non-distended abdomen with an obvious palpable mass located in the lower abdomen that was painful, firm, and tubular in shape with regular boundaries. An abdominal and pelvic CT with IV contrast was performed, showing a tubular-shaped foreign object retained within the abdominal cavity.
At this point, surgical retrieval of the foreign material was decided. During the surgical extraction, a 4 cm horizontal incision was made over the palpable lump that was positioned in the lower abdominal area. Then, the dissection of the abdominal wall layers was done, during which a tubular material was recognized, and complete extraction was achieved (Figure 1). Intraoperatively, the detected object was unintentionally retained drain from the abdominoplasty procedure that was performed 8 years ago (Figure 2). The postoperative period was uneventful. The patient was discharged home on postoperative day 1.
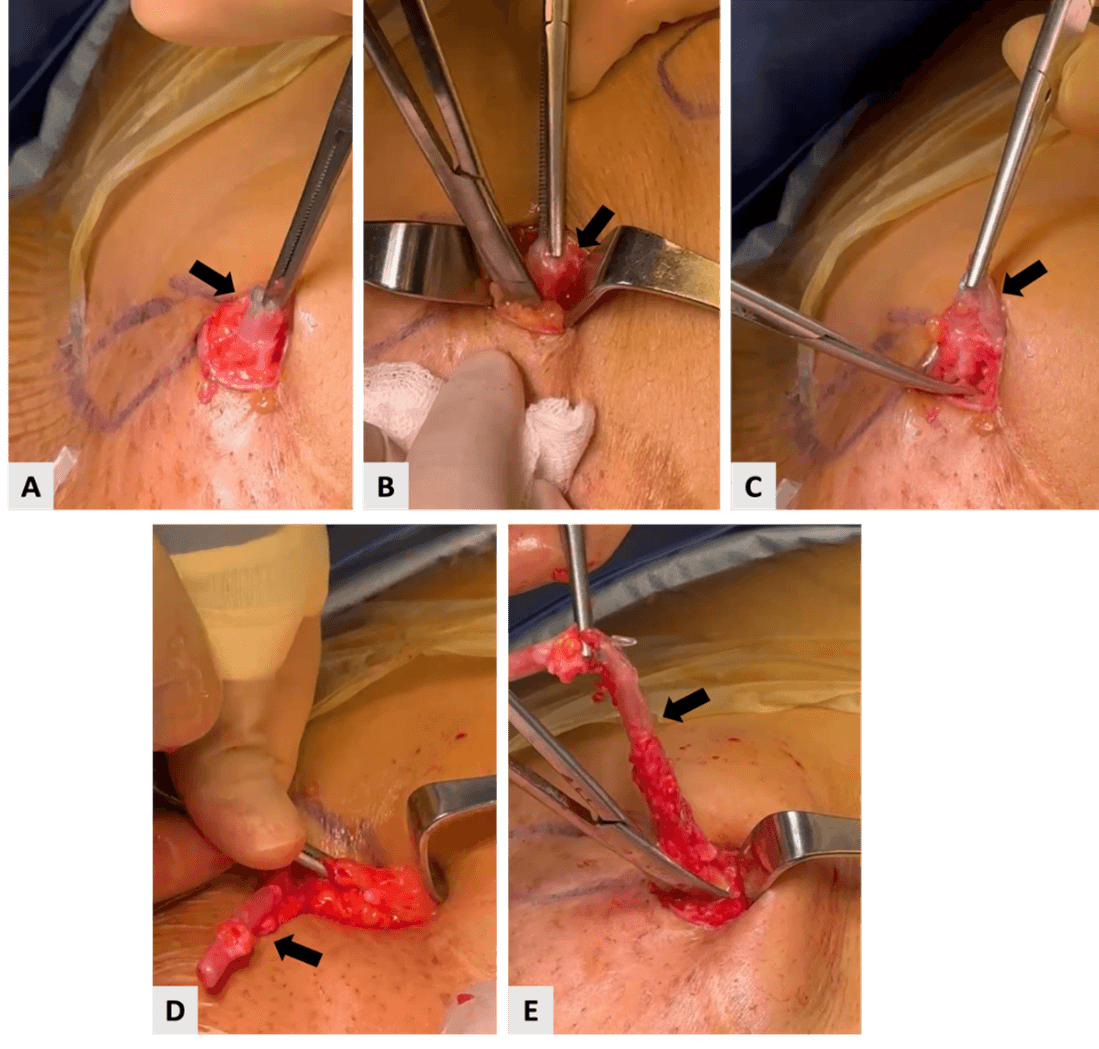
Figure 1: Treatment approach by open surgical technique. A-D) Showing surgical retrieval of the drain. The black arrow points to the retained drain.
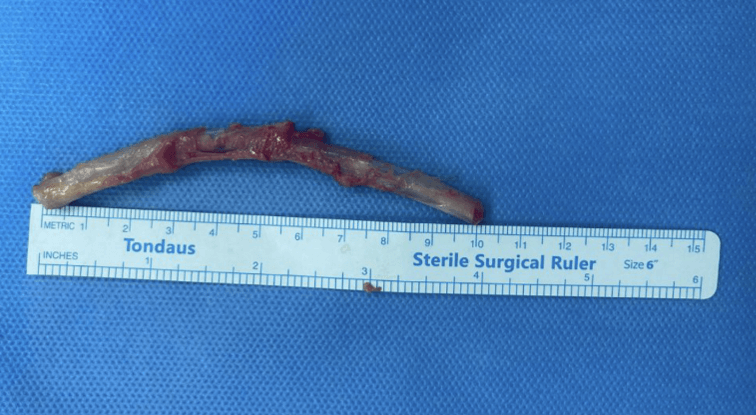
Figure 2: Surgically retained drain that was detected intraoperatively.
Discussion
Retained surgical bodies (RSB) can be defined as unintended retained foreign objects in the patient’s body [2]. The retention of these items following wound closure is uncommon, and avoidable, demanding special consideration as well as organizational preventative approaches [abd8]. Gauzes and swabs made of cotton are the most frequently retained materials, accounting for almost 70% of instances [7]. The thoracic and abdominal cavities are the most impacted regions as in our case the preserved object, a drain fragment, was detected within the abdominal cavity [7].
The position of the RSB influences the patient's clinical characteristics, which can manifest as acute, subacute, or absent symptoms [7]. The resultant symptoms originated from obstruction, compression, malnutrition, and/or microbial expansion [7, 8]. It is essential to recognize that individuals might experience postoperative signs and symptoms years following surgery. Thirty-three years after surgery, a laparotomy pad went through the colon in a documented case [8]. The patient in the current case presented with a long-standing history, of 8 years of painless abdominal mass.
Technical measures such as product calculating or marking, radio-frequency identification on surgical packs, and magnetized items for enhancing item measurements can all help improve RSB recognition and augment counts [5, 9]. In general, those kinds of cases of retained instruments post-surgery are clinically unexpected in a postoperative patient, most often recognized on imaging [10].
Plain films, gastrointestinal contrast tests, and CT scans are diagnostic tools for surgically retained bodies [1]. Usually, the unintentionally retained drains might be missed due to overstretching by excessive forces that can be used during drain removal or sutured loosely with an unsecured knot [8]. Our case demonstrated the role of abdominal CT in diagnosing and identifying the reserved fractured drainage tube.
Treatment is re-exploration and surgical removal of the retained material, including laparotomy [1, 7]. The treatment approach in the presented case was achieved after localizing the position of the retained drain fragment by a small abdominal incision with intraoperative details mentioned in the case presentation section.
Conclusion
Generally, the occurrence of RSBs is an uncommon event that is associated with serious consequences. Radiographic tools are used for RSB identification and detection. The establishment of a specific error reporting strategy is crucial to prevent RSB, increase awareness, and improve professional communication between surgical teams in the operating theatre.
Conflicts of Interest
None.
Funding
None.
Ethical Approval
Not applicable.
Consent
Written informed consent was obtained from the patient to publish this case report and accompanying images. On request, a copy of the written consent is available for review by the Editor-in-Chief of this journal.
Research Registration
Not applicable.
Provenance and Peer Review
Not commissioned, externally peer reviewed.
Author Contribution
Hamad Alsanea: assist in surgery, literature review, paper writing, and editing, picture editing. Athary Saleem: literature review, picture editing, paper editing, and manuscript drafting. Fahad Alhamadi: performed surgery, and paper editing. Mohammed Asad: performed surgery, critical review, supervision, and final approval.
Guarantor
Hamad Alsanea, M.D., General Surgery Department, Al-Adan Hospital, Kuwait.
Article Info
Article Type
Case ReportPublication history
Received: Mon 29, Jan 2024Accepted: Sat 17, Feb 2024
Published: Fri 01, Mar 2024
Copyright
© 2023 Hamad Alsanea. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.CRSS.2024.01.01
Figures & Tables
References
1. Zejnullahu VA, Bicaj
BX, Zejnullahu VA, Hamza AR (2017) Retained surgical foreign bodies after
surgery. Open Access Maced J Med Sci 5: 97-100. [Crossref]
2. National Quality
Forum. (2011) Serious reportable events in healthcare-2011 update: a consensus
report.
3. Düx M, Ganten M,
Lubienski A, Grenacher L (2002) Retained surgical sponge with migration into
the duodenum and persistent duodenal fistula. Eur Radiol 12:
S74-S77. [Crossref]
4. Lata I, Kapoor D,
Sahu S (2011) Gossypiboma, a rare cause of acute abdomen: A case report and
review of literature. Int J Crit Illn Inj
Sci 1: 157-160. [Crossref]
5. Hibbert PD, Thomas
MJ, Deakin A, Runciman WB, Carson Stevens A et al. (2020) A qualitative content
analysis of retained surgical items: learning from root cause analysis
investigations. Int J Qual Health Care
32: 184-189. [Crossref]
6. Agha RA, Franchi T,
Sohrabi C, Mathew G, Kerwan A (2020) The SCARE 2020 Guideline: Updating
Consensus Surgical CAse REport (SCARE) Guidelines. Int J Surg 84:
226-230. [Crossref]
7. Favarin GJS,
Favarin E, Borges AN, Pinto Junior AM, Baggio VA et al. (2023) Surgical item
left in the abdomen six years after abdominoplasty: case report. Revista Brasileira de Cirurgia Plástica 31: 583-585.
8. Klein J, Farman J,
Burrell M, Demeter E, Frosina C (1988) The forgotten surgical foreign body. Gastrointest Radiol 13: 173-176. [Crossref]
9. Gayer G, Lubner MG, Bhalla S, Pickhardt PJ (2014) Imaging of abdominal and pelvic surgical and postprocedural foreign bodies. Radiol Clin North Am 52: 991-1027. [Crossref]
10. Ahn JH, Kang CH, Choi SJ, Park MS, Jung SM et al. (2016) CT findings of foreign body reaction to a retained endoloop ligature plastic tube mimicking acute appendicitis: a case report. Korean J Radiol 17: 541-544. [Crossref]