Ileocecal Intussusception in an Adult Secondary to a Colon Adenocarcinoma: A Case Report and Literature Review
A B S T R A C T
Intussusception is defined as telescoping of a proximal segment of the gastrointestinal tract into a distal segment caused by an organic lesion usually on the bowel that functions as a guiding point been pulled towards a distal segment due to normal peristalsis. It is rare in adults, and it represents only 5% of all intussusceptions which for the most part has been reported in the rectosigmoid colon and mostly diagnosed during surgery. We present a patient with intermittent abdominal pain and intermittent mild symptoms of bowel obstruction who reveals in imaging studies an ileocecal intussusception and due to his age, loss of weight, and a palpable tumor, a malignancy as the cause of intussusception was suspected. The histopathological study reported a colon adenocarcinoma. Although it is possible to reduce an intussusception, this should be avoided in adults due to a high malignancy rate and a perforation risk of the piece that might cause tumor cell dissemination. Taking in consideration what has been reported in literature and the colon cancer epidemiology, we should always keep in mind the possibility of a malignant tumor in a colonic intussusception finding, regardless if it is diagnosed during preoperative by imaging studies in a scheduled patient or if it is found during an emergency laparotomy.
Keywords
Intussusception, colonic intussusception, colon cancer, colon tumor, adenocarcinoma of colon
Introduction
Although intussusception was first described by Paul Barbette as a proximal bowel invagination to a distal portion, it was John Hunter who coined the term “intussusception” in 1789 by describing three patients with such findings [1]. Presently it is defined as telescoping of a proximal segment of the gastrointestinal tract into a distal segment and it occurs when an organic lesion of the bowel functions as a guiding point and it is pulled towards a distal segment due to normal peristalsis [2-5].
It is rare in adults, and it represents only 5% of all intussusceptions and 1-5% of all bowel obstruction cases [1, 2, 4-12]. Unlike pediatric patients in whom it is generally idiopathic, in adults, over 90% are due to an established pathology [1, 7, 8]. We present a case of a patient with ileocecal intussusception secondary to a colon adenocarcinoma.
Case Presentation
No relevant personal history background 80-year-old male who attends checkup complaining of intermittent abdominal pain, lack of appetite, not quantified loss of weight, constipation and self-perception of an abdominal tumor. After physical examination, a tumor in the right lower abdomen could be touched, rest of the examination without further abnormalities. Bloodwork reports hemoglobin 11 g/dL, white blood cells 9500/mm3, creatinine, glucose, liver function test and coagulation tests in normal parameters. Abdomen computed tomography (CT) shows thickening of the ascending colon walls compatible with a colonic intussusception with no suspicious mesenteric adenopathies or metastatic activity (Figure 1). Having in mind the patient’s age, his symptoms and CT findings, carcinoembryonic antigen test was ordered and reported in 3.1 ng/mL.
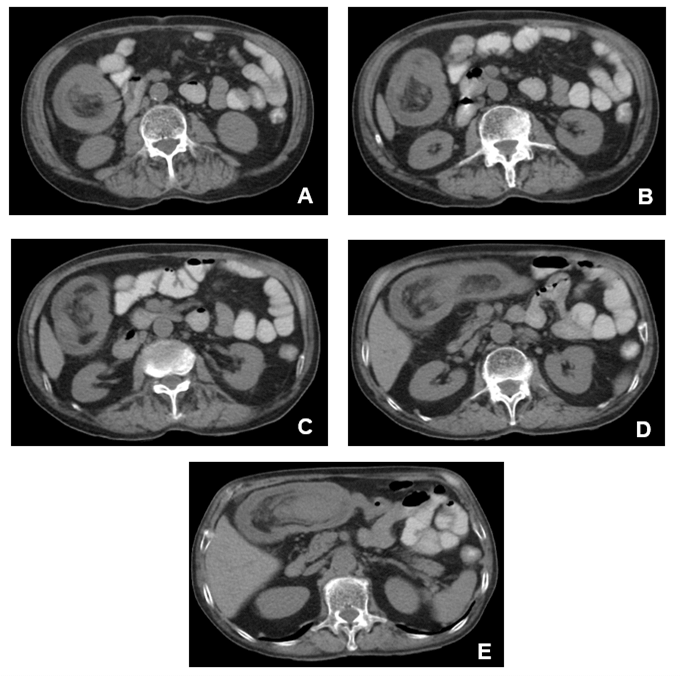
Figure 1: Ileocecal intussusception showing in a way of sequencing the introduction of the ileum and the cecum into the ascending colon with no suspicious mesenteric adenopathies nor metastatic activity and thickening of the colon walls with the appearance of a three-layer structure conformed by bowel wall, mesentery and trapped bowel.
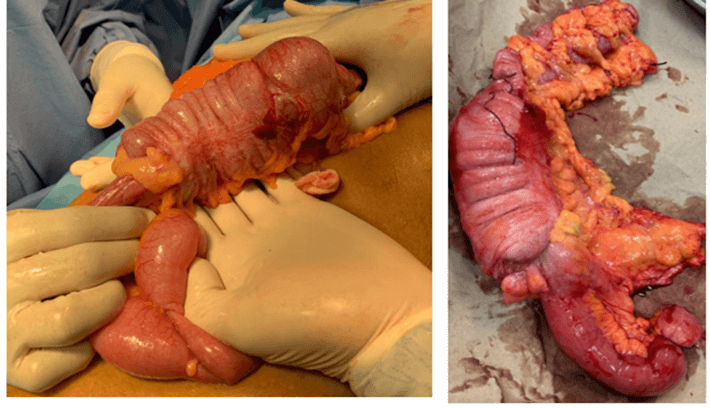
Figure 2: Ileocecal intussusception resected as a right radical hemicolectomy without attempted reduction.
An exploratory laparotomy was performed, finding a cecum tumor with intussusception to the ascending colon (Figure 2). Therefore, we decided to perform a radical right hemicolectomy with ileotransverse side to side anastomosis without intussusception reduction. The histopathological study reported a moderately differentiated adenocarcinoma invading muscularis propria, without lymphovascular invasion and sixteen non-metastatic regional lymph nodes, staging tumor as a T2N0M0 EC I. The patient had a good recovery after surgery, with good oral tolerance and was discharged 4 days after the procedure.
Discussion
Any bowel alteration that leads to a change in normal peristalsis pattern increases an intussusception risk. Based on location and guiding point to its development, intussusception may be classified in enteric (limited to small bowel segment), ileocolic (from ileum to colon), colonic (colon to colon) and ileocecal (ileum and cecum to ascending colon); this last type was presented by our patient secondary to a cecum tumor [1, 5]. Most colon intussusceptions occur in flexible segments like sigmoid, transverse colon and cecum since both ascending and descending colon are attached to retroperitoneum [5, 9, 12, 13]. During our search, we found that most cases of colon tumors with intussusception were reported in the rectosigmoid colon, and only two cases were reported in the right colon, mainly at the cecum [8]. Moreover, the most frequent development mechanism is anterograde, and the retrograde mechanism occurs in less than 1% of cases [8].
52-55% of intussusceptions occur in the small bowel, and whenever it is caused by a tumor, 80% of these are benign [7, 13]. Only 15-27% of intussusceptions develop in the colon and in 65-77% of cases, a malignant tumor is the cause, which are mostly diagnosed during surgery [1, 6, 7, 9, 13]. However, in our review, some cases indeed reported preoperative diagnosis of intussusception by imaging tests like our patient. While in colon adenocarcinoma is the most common tumor in an intussusception, the most frequent benign tumor that acts as a guiding point for intussusception both in small bowel and colon is submucosal lipoma, which prevails in the cecum followed by the ascending colon and the sigmoid colon; other causes include polyps, leiomyomas, Meckel’s diverticulum, adhesions, Crohn's disease, inflammatory pseudotumor, intestinal lymphoma, appendix tumors and in few cases, it could be idiopathic in adults [1, 3, 4, 7, 14-16]. Lastly, a greater number of pediatric and adult patients with cystic fibrosis had been reported with intussusceptions, being in these patient ten times more frequent than the rest of the population [17].
Concerning age, intussusception is more frequent after the fifty years of age. Most cases in our review were patients over 60 years old; this could be related to the presentation age of malignant colon tumors which are the main cause. However, there are reported cases in patients of less than 40 years old and it seems to be more common in women (H:M relation 1:5) [1, 11].
Regarding its presentation, intussusception has no specific symptoms, and unlike in children, the classic triad of abdominal pain, bloody diarrhea and a palpable tumor, hardly ever happens in adults [3, 4, 7, 9, 12]. The most frequent symptom is abdominal pain, which presents persistently and sometimes may be accompanied by intermittent symptoms of bowel obstruction (nausea, vomiting, distention and constipation). Therefore, whenever a patient presents with periodic complaints of abdominal pain and intermittent bowel obstruction symptoms, intussusception should be included in the differential diagnosis [1, 4, 12]. Less than 20% of patients show up with acute abdomen due to intestinal obstruction, and since in this scenario, its more difficult to reach a diagnosis in the preoperative stage, we should always suspect malignancy when finding an intussusception during surgery [1, 3, 8, 9]. Our patient presented with chronic symptomatology, and due to his age, loss of weight and a palpable tumor, a malignancy as the cause of intussusception was suspected.
Because of the diverse presentation of symptoms, and that we cannot always see the characteristic images of intussusception in imaging test during the preoperative stage, the intussusception preoperative diagnostic rate is only 40-50% [2, 7]. Abdomen x-ray usually reveals signs of bowel obstruction; on the ultrasonography, the characteristic intussusception image is a hyperechogenic concentric double halo finding along with thickening of the intestine wall [7, 13]. Most reports describe the CT as the most sensitive diagnostic test, the characteristic images include bulls eye sign and the appearance of a three-layer structure conformed by bowel wall, mesentery and trapped bowel [1, 3, 7, 9, 12]. Other diagnostic methods include barium enema and colonoscopy, which could be cause-revealing and could even reduce intussusception [1].
Although there are reports stating that by having an intussusception diagnostic by imaging studies like CT it is possible to offer a conservative treatment having close follow up, serial imaging studies and endoscopy surveillance, most authors report that laparotomy is mandatory due to high chances of finding the origin of intussusception as a lesion that could be malignant [4].
Although it is possible to reduce an intussusception, this should be avoided due to a high malignancy rate and perforation risk of the piece that might cause tumor cells dissemination [1, 2, 5, 7, 9, 12, 13, 18]. Some authors recommend that the decision of reducing the intussusception before performing resection, or performing resection without reducing it during surgery, must be taken by the surgeon on the spot based on its location (small bowel or colon), the presence or absence of ischaemia, a malignancy suspicion, evolution time, and the length of affected bowel, especially in small bowel [1, 2, 4]. In addition, the decision of performing an anastomosis after resection will rely on the bowel conditions and the general performance of the patient [5]. At last, there are reports of successfully intussusception reductions secondary to tumors by colonoscopy [19].
Conclusion
Intussusception in adults is uncommon, and most of them are the consequence of tumors. This fact alone is the main reason why an exploratory laparotomy should be performed to reach a resolution and find its origin. Taking in consideration what has been reported in literature and the colon cancer epidemiology, we should always keep in mind the possibility of a malignant tumor in a colonic intussusception finding, regardless if it is diagnosed during preoperative imaging studies of the scheduled patient or if it is found during an emergency laparotomy. In addition, due to the high chances of a malignant cause, in adults, reduction attempts should be avoided unless there is a low suspicion of perforation and malignancy, few irreversible intestinal ischaemia signs and or the affected bowel segment is long enough or too close to the ligament of Treitz to put on doubt its resection.
Conflicts of Interest
None.
Funding
None.
Article Info
Article Type
Case Report and Review of the LiteraturePublication history
Received: Wed 17, Jun 2020Accepted: Tue 30, Jun 2020
Published: Wed 30, Sep 2020
Copyright
© 2023 Carlos Hernández Brito. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.AJSCR.2020.03.03
Figures & Tables
References
- Honjo H, Mike M, Kusanagi H, Kano N (2015) Adult Intussusception: A Retrospective Review. World J Surg 39: 134-138. [Crossref]
- Saigusa S, Ohi M, Imaoka H, Shimura T, Inoue Y et al. (2014) Intussusception of Rectosigmoid Colon Cancer Mimicking a Pedunculated Tumor. Case Rep Surg 2014: 696403. [Crossref]
- Asokan G, Hollington P (2014) Sigmoid malignancy presenting as recto-sigmoid intussusception. ANZ J Surg 84: 386-393. [Crossref]
- Dan JM, Agarwal S, Burke P, Mahoney EJ (2012) Adult intussusception secondary to colorectal cancer in a young man: a case report. J Emerg Med 43: 983-986. [Crossref]
- Sun K, Yang D, Gan M, Wu X (2015) Descending colo-colonic intussusception secondary to signet ring cell carcinoma: A case report. Oncol Lett 9: 1380-1382. [Crossref]
- Chiba H, Takahashi A, Inamori M, Goto T, Ohata K et al. (2014) Early colon cancer presenting as intussusception and successfully treated using endoscopic submucosal dissection. Endoscopy 46: E326-E327. [Crossref]
- Chen C, Lai C, Hsiao K (2012) Synchronous adenocarcinomas of the colon presenting as synchronous colocolic intussusceptions in an adult. World J Surg Oncol 10: 272. [Crossref]
- Chand M, Bradford L, Nash GF (2008) Intussusception in Colorectal Cancer. Clin Colorectal Cancer 7: 204-205. [Crossref]
- Fukuchi M, Tsukagoshi R, Sakurai S, Suzuki M, Naitoh H et al. (2012) Adult Intussusception Caused by Descending Colon Cancer during Chemotherapy of Stomach Cancer Recurrence. Case Rep Gastroenterol 6: 88-93. [Crossref]
- Ramesh R, Juhn A, Babey M, Patel K, Liu B (2016) An Unusual Case of Colonic Intussusception Masquerading as a Transverse Colon Mass. Am J Gastroenterol 111: 921. [Crossref]
- Vemuru SR, Friel CM, Hoang SC (2018) Adenocarcinoma as the Lead Point Leading to Colo-Colic Intussusception. J Gastrointest Surg 22: 2177-2178. [Crossref]
- Xu X, Hong T, Liu W, Zheng C, He X et al. (2013) A long adult intussusception secondary to transverse colon cancer. World J Gastroenterol 19: 3517-3519. [Crossref]
- Yol S, Bostanci EB, Özoğul Y, Akoğlu M (2004) Extensive Adult Colo-Colonic Intussusception From Ascending Colon to Sigmoid Colon: Report of a Case. Turk J Gastroenterol 15: 201-203. [Crossref]
- Gluskin AB, Singh NA (2017) Gastrointestinal: A sigmoid lipoma as the cause of Intussusception. J Gastroenterol Hepatol 32: 292. [Crossref]
- Huang Y, Li L, Wang J, Lun Z, Li W et al. (2015) Inflammatory pseudotumor of the colon causing intussusception: A case report and literature review. World J Gastroenterol 21: 704-710. [Crossref]
- Xu X, Kong Z, Yi K, Wang B, Lei Q et al. (2019) Colonic Mucinous Adenocarcinoma Causing Intussusception and Distant Metastasis: A Case Report. Medicine (Baltimore) 98: e15740. [Crossref]
- Gilchrist FJ, Jones AM, Bright Thomas RJ (2012) Intussusception and metastatic colon cancer in an adult with cystic fibrosis. J R Soc Med 105: S40-S43. [Crossref]
- Chuah YY, Lee YY, Shih CA (2017) Adult primary medullary carcinoma: an unusual cause of pain from intussusception. Br J Hosp Med (Lond) 78: 474. [Crossref]
- Hsu W, Lu C, Hu H (2015) Sigmoid colon cancer with intussusception reduced by Colonoscopy. Gastrointest Endosc 82: 753. [Crossref]