Kinking of Disposable Fiberoptic Bronchoscope During Difficult Nasal Awake Intubation
A B S T R A C T
Background: disposable fiberoptic for intubation are more and more available in operating room We hereby report a complication of a difficult fiberoptic intubation performed with a disposable fiberscope.
Case: Under remifentanil sedation Visualizing the glottis was easy while advancing the endotracheal tube through the fiberscope was mildly difficult. Removing the fiberscope was impossible as was the removal of the endotracheal tube. The patient was becoming uncomfortable. Under local anesthesia we performed a jet ventilation after puncture of the cricothyroid membrane followed by total intravenous anesthesia. A cervicofacial surgeon visualized the kinking of the fiberscope at the tip of the endotracheal tube. The fiberscope was removed under direct vision with a rigid bronchoscope.
Conclusion: Because of more flexibility disposable fiberscopes may kink during the introduction of the endotracheal tube.
Keywords
disposable fiberscope, difficult intubation, rescue jet ventilation
A 28 years old female suffering from pharyngeal cancer had a history of a first long lasting (9h) surgery with oropharyngeal free flap harvested from the anterior right thigh followed by a postoperative tracheotomy (72h). At postoperative day 10 a second surgery was needed in order to perform some additional sutures to close a pharyngeal fistula. During the anesthetic assessment a probable difficult intubation was predicted mainly because of the size of the free flap and the closure of the tracheotomy, thus an awake fiberoptic intubation was decided for management of difficult airway. The right nostril was chosen as it was already used for the first surgery , oropharyngeal intubation was dismissed because of the site of surgery.
After local anesthesia of the right nostril and the pharyngeal posterior wall , a target infusion of Remifentanil was started ( average target 2.5 ng/ml). A disposable adult Ambu® fibroscope 2 was used and a armed flexible 6.5 mm tracheal tube was mounted after lubrification. Locating the glottis was mildly difficult probably because of the swelling of the free flap in the oropharynx, however the fiberscope could pass easily the glottis after local anesthesia injected through the fibroscope. The tracheal tube was advanced under visual guidance above the carina, the passage of the tracheal tube was also mildly difficult, the patient coughed several times, despite local anesthesia and remifentanil sedation the carina was still visible after introduction and the tracheal entry.
After the tracheal tube insertion, we noticed that removing the fibroscope was not possible, however pushing forward either of fiberscope or the tube was possible but did not permit subsequently to pull out the fiberscope neither the tracheal tube. After several forward or backward attempts further manipulation became impossible , the patient maintained an adequate saturation but started to feel very anxious and uncomfortable, we also re-attempted to withdraw the tube, however this attempt appeared to be very painful for the patient and necessitated unusual traction force. Therefore, we decided not to insist on removing it in order to not possibly damage the airway or adjacent structure including the free flap and decided to secure another airway via inter crico-thyroid membrane puncture under local anesthesia using the previous tracheotomy scar [1]. This permitted to secure oxygenation by a Monsoon® jet ventilator through a 14G catheter and put the patient to sleep under propofol, remifentanil and succinylcholine.
A cervicofacial surgeon performed a laryngoscopy followed by a bronchoscopy with a rigid tube and noticed the kinking of the fiberscope at the tip of the tracheal tube and further and the end of the fibrescope which was slipped in a main left bronchi (Figure 1) probably during secondary manipulation in order to remove either the fiberscope and or the tracheal tube. After verifying all anatomic aspect , the tube was pushed backward until the fiberscope was removed from the main left bronchi and then under direct bronchoscopic vision once we were assured that the airway and the freeflap could not be damaged at the same time.
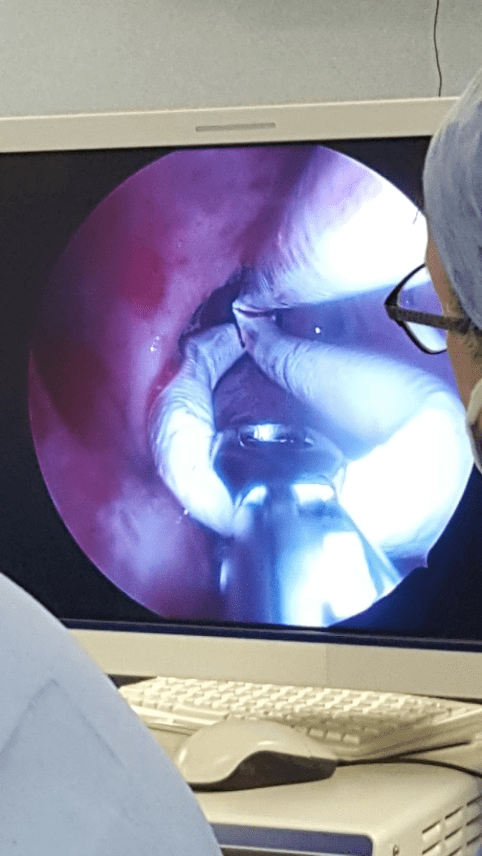
Figure 1:
At the end of surgery, the previous tracheotomy was reopened to avoid discomfort and risk of edema after the airway manipulation and the swelling of the oropharynx due to the freeflap which was sutured to adjacent structures. Disposable fiberoptic bronchoscope are becoming more and more popular [2, 3]. We believe this complication would happen more frequently and more severely with a single use fiberoptic bronchoscope(4) as traditional fibroscope are more rigid and less flexible while the intubation could have been more difficult with the latter one . We did not routinely checked the structural integrity of the fibroscope before operation but we believe the kinking occurred probably during the intubation maneuver while trying to pass the tube through the fibroscope in the pharynx as this part of fiberoptic intubation is the second delicate part of the fiberoptic intubation during maneuvers [4]. Pushing forward the fibrescope created deviation of the tip of the fiberscope through left main bronchi and and blocked the whole fibroscope in the trachea. In addition, we cannot rule out mild kinking before maneuvers , therefore structural integrity of these disposable device should be checked before operation and finally kinking of such devices during the procedures should be kept in mind and especially when pushing forward in case of blockade.
Article Info
Article Type
Case ReportPublication history
Received: Wed 21, Aug 2019Accepted: Tue 08, Oct 2019
Published: Sat 09, Nov 2019
Copyright
© 2023 Cyrus Motamed. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.GCCR.2019.01.03
Figures & Tables
References
- Abernathy JH 3rd, Reeves ST (2010) Airway catastrophes. Curr Opin Anaesthesiol 23: 41-46. [Crossref]
- Aissou M, Coroir M, Debes C, Camus T, Hadri N et al. (2013) [Cost analysis comparing single-use (Ambu(R) aScope) and conventional reusable fiberoptic flexible scopes for difficult tracheal intubation]. Ann Fr Anesth Reanim 32: 291-295. [Crossref]
- Videau M, Rghioui K, Mottet B, Sainfort A, Lefort I (2017) [A comparative cost analysis of single-use versus reusable fiberoptic bronchoscopes: Is single-use fiberscope worth it?]. Ann Pharm Fr 75: 473-479. [Crossref]
- Asai T, Shingu K (2004) Difficulty in advancing a tracheal tube over a fibreoptic bronchoscope: incidence, causes and solutions. Br J Anaesth 92: 870-881. [Crossref]