Meckel’s Diverticulum in Foramen of Winslow Hernia – A Rare Cause of Bowel Obstruction
A B S T R A C T
Foramen of Winslow hernia is a rare cause of bowel obstruction, historically linked to high morbidity and mortality. With the progression of high-resolution imaging devices, the early diagnosis of this pathology can be safely made. This has caused significant improvement in outcomes, where prompt surgical reduction can be readily organized. There has, however, not been any reported case of Meckel’s diverticulum driving this internal hernia. This is a case report of a foramen of Winslow hernia (FOWH) containing a Meckel’s diverticulum, managed via laparoscopic reduction of hernia contents and diverticulectomy.
Keywords
Bowel obstruction, foramen of Winslow, Meckel’s diverticulum
Introduction
Foramen of Winslow hernia is a rare cause of bowel obstruction, historically linked to high morbidity and mortality. With the progression of high-resolution imaging devices, the early diagnosis of this pathology can be safely made. This has caused significant improvement in outcomes, where prompt surgical reduction can be readily organized. There has, however, not been any reported case of Meckel’s diverticulum driving this internal hernia. This is a case report of a foramen of Winslow hernia (FOWH) containing a Meckel’s diverticulum, managed via laparoscopic reduction of hernia contents and diverticulectomy.
Case Report
A 76 year-old male presented to the emergency department with a 1-day history of cramping abdominal pain associated with bloating and constipation. The pain woke him from sleep, worsening progressively throughout the day. That prompted him to present to the emergency department for assessment. The bowels last opened the day before, not passing flatus since the beginning of the pain. The paient reported feeling full, with nausea, but denied vomiting. He denied septic symptoms and had been feeling well 24h prior to the start of symptoms.
The patient’s medical background consisted of ischemic heart disease (previous Coronary Artery Bypass Graft surgery) and dyslipidemia, for which the patient was on daily aspirin. His surgical background consisted of melanoma excision (torso), open left hernia inguinal repair with mesh and open appendicectomy. On initial assessment, the patient had unremarkable vital signs, with an abdominal examination of a soft distended abdomen, with mild guarding centrally. No peritonism was reported. His blood results were within the normal range. Based on previous surgical history, concern was raised of small bowel obstruction, and an urgent abdominal computed tomography (CT) readily organized. The scan results showed a small bowel loop trapped between the stomach and the liver, protruding through the Epiploic foramen, with clear features of a foramen of Winslow herniation (Figure 1). There were no signs of bowel compromise then.
The decision was made to perform a laparoscopic reduction of small bowel obstruction, provided the respective bowel loop looked healthy and uncompromised, with the possibility of bowel resection and conversion into laparotomy if necessary. During laparoscopic assessment, an ileal loop was found to be herniating through the Epiploic foramen (Figure 2) that was reduced. During reduction, a Meckel’s diverticulum was seen at the herniated ileal loop (Figure 3). A diverticulectomy was then performed, with a 60mm laparoscopic GIA stapler in a tangential fashion. The patient had an uneventful postoperative recovery, being discharged from hospital on day 4 post-procedure. At one-month follow-up appointment, histology was reviewed, and it confirmed Meckel’s diverticulum without the presence of heterotopic tissue. No malignancy was identified. There have been no further obstructive issues, with the patient being discharged from the general surgeon’s clinic.

Figure 1: CT showing small bowel loop trapped through Epiploic foramen, consisting of foramen of Winslow hernia.
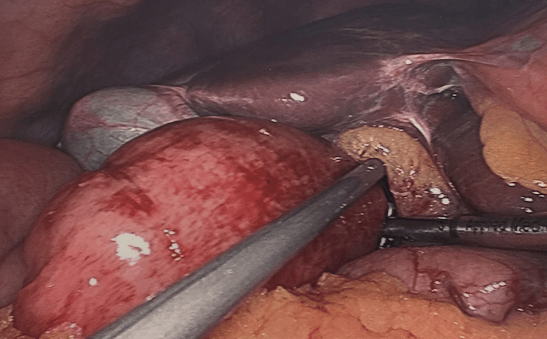
Figure 2: Laparoscopic finding of herniated small bowel loop through foramen of Winslow.
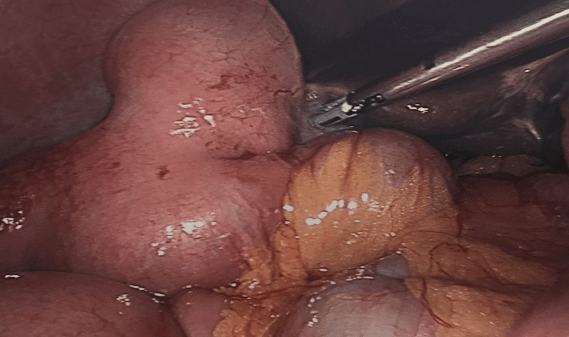
Figure 3: Laparoscopic finding of Meckel’s diverticulum in herniated small bowel loop.
Discussion
FOWH accounts for 0.08% of all visceral hernias and 8% of bowel obstruction secondary to internal hernias [1, 2]. Historically FOWH was considered difficult to diagnose, often resulting in strangulated bowel contents at the time of presentation [3, 4]. This was associated with a high mortality rate of up to 50% before the advent of more reliable imaging resources [2]. Luckily this has changed quite significantly with the advent of high-resolution imaging tools. Easily accessible imaging investigations (i.e., computed tomography) have made accurate diagnosis and early operative management possible, drastically decreasing the mortality rate to 5% [2]. The laparoscopic approach has been more frequently reported in recent papers [2-5]. This is likely to be due to the early assessment and diagnosis, resulting in more stable patients, who are suitable for a minimally invasive operation in contrast to exploratory laparotomy. Widespread access to laparoscopic equipment, as well as widely disseminated laparoscopic training also plays an important role [5, 6]. There has been some discussion as to whether to perform prophylactic surgical measures to prevent recurrence (foramen closure), with insufficient data to support either [2, 7].
Meckel’s diverticulum is a true congenital diverticulum, which is present in around 2% of the population and is a remnant of the omphalomesenteric duct [8]. This diverticulum is located within 60cm of the ileocecal valve, in the antimesenteric border of the small bowel. Of those who have the diverticulum, the lifetime risk of complication is approximately 4% [9]. The commonest complication in adult patients is obstruction, followed by bleeding [8]. Diverticulectomy is the well-established treatment of choice for symptomatic Meckel’s diverticulum. It can be achieved with three distinct operative techniques – segmental resection-anastomosis, wedge resection, or tangential stapling [10]. In this case, we opted for tangential stapling, given the bowel viability. To our knowledge, there has not been reported in the literature a case of FOWH containing Meckel’s diverticulum.
Conclusion
Foramen of Winslow hernia is a rare cause of internal hernia, with distinct radiological features. Early recognition of this pathology is imperative for a good prognosis. Laparoscopic reduction is currently the most appropriate treatment option, provided there’s no bowel ischemia. To our knowledge, there has been no previous case reports of FOWH caused by a Meckel’s diverticulum.
Article Info
Article Type
Case ReportPublication history
Received: Thu 23, Jan 2020Accepted: Wed 12, Feb 2020
Published: Fri 21, Feb 2020
Copyright
© 2023 Maria Julia Corbetta Machado. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.IJSCR.2020.01.05
Figures & Tables
References
- Downs P, Downes N, Zayshlyy E, Esper C, Giuseppucci P (2018) Internal hernia through foramen of Winslow. J Surg Case Rep 2018: rjy329. [Crossref]
- Brandão PN, Mesquita I, Sampaio M, Martins P, Daniel J et al. (2016) Foramen of Winslow hernia: a case report of a minimally invasive approach. J Surg Case Rep pii: rjw205. [Crossref]
- Sikimininywa Kambale P, Anaye A, Roulet D, Pezzetta E (2014) Internal hernia through the foramen of Winslow: a diagnosis to consider in moderate epigastric pain. J Surg Case Rep pii: rju065. [Crossref]
- Daher R, Montana L, Abdullah J, d’Alessandro A, Chouillard E (2016) Laparoscopic management of foramen of Winslow incarcerated hernia. Surg Case Rep 2: 9. [Crossref]
- Garg S, Flumeri Perez G, Perveen S, DeNoto G (2016) Laparoscopic repair of foramen of Winslow hernia. Int J Angiol 25: 64-67. [Crossref]
- Harnsberger CR, McLemore EC, Broderick RC, Fuchus HF, Yu PT et al. (2015) Foramen of Winslow hernia: a minimally invasive approach. Surg Endosc 29: 2385-2388. [Crossref]
- Moris D, Tsilimigras DI, Yerokun B, Seymor KA, Guerron AD et al. (2019) Foramen of Winslow Hernia: a Review of the Literature Highlighting the Role of Laparoscopy. J Gastrointest Surg 23: 2093-2099. [Crossref]
- Luu AM, Meurer K, Herzog T, Uhl W, Tannapfel A et al. (2016) Small bowel obstruction due to a giant Meckel’s diverticulum. Visc Med 32: 434-436. [Crossref]
- Capelão G, Santos M, Hilário S, Laureano M, Nobre J et al. (2017) Intestinal Obstruction by Giant Meckel’s Diverticulum. GE Port J Gastroenterol 24: 183-187. [Crossref]
- Lequet J, Menahem B, Alves A, Fohlen A, Mulliri A (2017) Meckel’s diverticulum in the adult. J Visc Surg 154: 253-259. [Crossref]