Metastasizing Ameloblastoma: A Systematic Review in Search of Clinicopathological Predictors
A B S T R A C T
Introduction: Ameloblastoma is a benign odontogenic tumor that is aggressive and localised in nature, listed as the first or second most prevalent odontogenic tumor and rarely tends to metastasis, but when it does, it receives the definition adopted by the WHO in 2017 of metastasizing ameloblastoma.
Materials and Methods: This systematic review of clinical case reports of metastasizing ameloblastoma from the last 10 years, collected from PubMed, ScienceDirect and Cochrane digital databases, aims to search for association between clinical/pathological and/or molecular parameters of ameloblastoma and its metastatic potential.
Results: The targeted search yielded 14 publications with a total of 18 clinical cases, which showed a mean age for diagnosis of metastasizing ameloblastoma of 46 years, with no gender predilection and a high probability of occurrence in the yellow Asian race, favouring a pattern of distant dissemination. The highest frequency of metastasis was associated with mandibular primary lesions diagnosed in young patients, and the most frequently found variant was the multicystic solid type, follicular subtype; distant metastasis was the predominant form of presentation, with the lungs being the main target.
Conclusion: At the moment, there is nothing that can predict metastatic potential in ameloblastoma. More standardised studies exploring the molecular terrain are needed, as this is a key and understudied factor.
Keywords
Ameloblastoma, metastasis, metastasizing
Introduction
Ameloblastoma (AM) is a benign neoplasm of odontogenic epithelium originating from residual epithelial components (Malassez's and reduced enamel organ remains), basal cells of the epithelium of the jaws and of the epithelium of cysts and benign odontogenic tumors such as dentigerous cyst and odontoma respectively; characterised by slow growth, aggressive local behaviour and high recurrence [1-3]. Despite being an infrequent pathology, representing 1% of all tumors in the head and neck region, with an estimated annual incidence of around 0.6 cases per million inhabitants, it is the first or second most prevalent odontogenic tumor in Latin America, varying according to the region [4]. A local study carried out at the Eugenio Espejo Hospital in the city of Quito, Ecuador, found ameloblastoma to be the most prevalent odontogenic tumor, followed by odontoma; epidemiology concordant with references from Brazil [4, 5].
The latest edition of the WHO for odontogenic tumors reformulates the classification of this tumor into 4 subtypes according to location and histological variant: 1) conventional AM (solid/multicystic type) representing 80% of cases, 2) unicystic AM, representing 5-15% of cases, 3) extraosseous peripheral AM, with less than 1% of cases and 4) metastasizing ameloblastoma (MA). Additionally, conventional and unicystic AM present histological sub-variants: follicular, plexiform, desmoplastic, acanthomatous, basal cell, granular cell within the conventional ones; and luminal, intraluminal, and mural variants for the unicystic forms [6]. Although conventional AM is the most prevalent and recurrent, metastatic ameloblastoma has demonstrated significant morbidity and mortality, especially in distant metastatic forms [7]. Indeed, after diagnosis of metastatic ameloblastoma to lung a medium survival of three years has been reported, and a 5-year survival rate for the same entity of 37% [8].
There is little research on this unusual pathology, which clinically presents as a malignant tumor but histologically appears as a benign tumor; the systematic reviews that have been published so far on the subject focus on the clinical-demographic aspects of this tumor, and the impact of these factors on the survival of the tumor once it has developed [6]. To date, there are no systematic reviews that focus on the clinicopathological and especially molecular factors that allow prediction of the type of AM that will evolve to a metastatic phenotype; we need more research, with a high level of evidence, that provides more information on the clinicopathological and molecular factors that help predict the development of this clinicopathological entity of complex biology. Against this background, our aim is to present a systematic review of clinical case reports of metastasizing ameloblastoma (MA) published in the last 10 years. The results of this research will provide head and neck clinicians with better tools in the prognostic assessment of patients diagnosed with ameloblastoma.
Materials and Methods
I Peak Question
Is it possible to predict the metastatic potential of ameloblastoma by clinicopathological and/or molecular markers?
II Eligibility or Inclusion Criteria and Data Extraction
Case reports and/or case series reporting clinical, pathological and/or molecular data on metastasizing ameloblastoma, published from 2011 to 2020, were included for this review. From each selected study, the following clinical data were taken: age, sex, comorbidities, toxic habits, history of human papillomavirus (HPV) and Epstein Barr virus (EBV) infections, tumor size, tumor location and radiographic appearance. The pathological and molecular data recorded from each selected study corresponded to histological variant and sub-variant of ameloblastoma, surgical margins, immuno-expression for MAPK (RAS, BRAF, FGFR2) and non-MAPK (SMO) oncogenes, proliferative marker Ki67, markers of inflammation such as COX2, markers of invasion such as metalloprotease (MMP) genes, tumor suppressors such as p53, and markers of epithelial-mesenchymal transition (E-cadherin, Syndican-1) [6, 9, 10].
III Exclusion Criteria
Letters to the editor, review articles, association articles, systematic reviews, clinical trials and articles that do not focus on the subject matter. In addition, scientific papers in incomplete text or without access were excluded.
IV Search Strategy
Based on the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines, an electronic search was conducted in three digital databases, PubMed, Science Direct and Cochrane for the collection of scientific articles published during the period 2011-2021, for which, MeSH terms were used in all fields, in order to maximise the search during the research [11, 12]. The search strategies defined for the databases described above were: metastasizing "AND" ameloblastoma OR metastases "AND" ameloblastoma "AND" clinical and pathological markers "OR" molecular markers "AND" case report. Only English language publications were considered, and duplicate articles in more than one database were considered only once.
V Study Selection
14 case reports were selected from the last ten years that provided information on the different variables established in the present study. Figure 1 details in flow chart the stages of the search process, filtering by exclusion criteria, and selection of studies according to eligibility criteria. Table 1 shows a summary of the number of studies obtained and excluded by database used in this study.
Table 1: Summary of the total number of studies obtained and filtered by
scientific database used in the study.
|
DATABASE |
Total publications |
Excluded by language |
Not relevant |
Incomplete text |
Total including |
|
PubMed |
82 |
0 |
55 |
16 |
11 |
|
ScienceDirect |
275 |
0 |
267 |
4 |
3 |
|
Cochrane |
7 |
0 |
7 |
0 |
0 |
VI Data Recording
The data were organized and processed in tables using Microsoft Excel 2010 software; statistical analysis was carried out by InfoStat software version 2018 of the National University of Cordoba, for which, a p-value of less than alpha error was considered significant, assuming as alpha a value equal to 0.05.
Results
I Demographic and Clinical Characteristics Associated with MA
Eighteen cases of metastasizing ameloblastoma (MA) were retrieved from a total of 14 published case reports on this pathological entity and selected under the pre-established inclusion and exclusion criteria (Figure 1 & Table 2). In our analysis, the metastatic tumor showed equal distribution in both sexes, with a mean age at diagnosis of 46 years and a clear predilection for the Asian yellow race. 77% of published cases reported mandibular location for the primary tumor, with the preferred site of metastasis being the lung, followed by cervical lymph nodes, and one case reported metastasis to multiple distant sites. The most common form of metastasis presentation was distant dissemination with 77.7% of the published cases, while loco-regional metastasis was the most infrequent form of MA manifestation (Table 3). Information on the diameter of the primary tumor was obtained in only 5 patients out of the 18 cases retrieved, with an average value of 3.5 cm for this variable. Regarding the radiographic appearance of the initial lesion, information was collected in only 8 of the 18 patients included in the study, with a clear predominance of radiolucent/hypodense multiloculated radiographic presentation and/or with irregular borders. In less than 25% of cases the presentation was uniloculated radiolucent, and only 12.5% of cases reported diffuse opacity based radiographic presentation (Table 3).
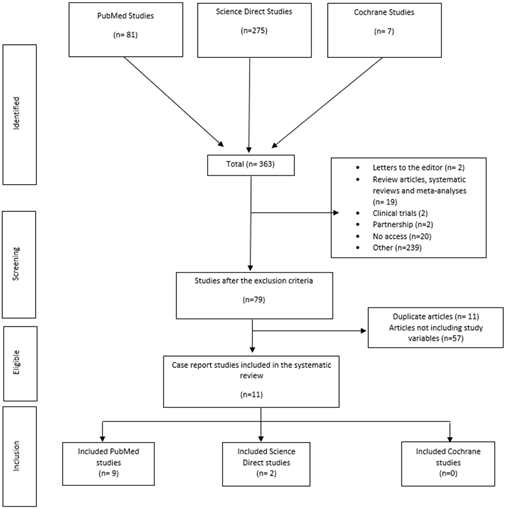
Figure 1: Flow chart showing the methodology used in the selection of studies for full analysis.
Table 2: List of studies with their respective clinical cases reported and
selected under the inclusion criteria established in this review.
|
Study |
Reference Number |
Number of clinical cases reported |
Level of evidence and recommendation according to SIGN [13] |
|
A case of ameloblastoma with extensive pulmonary metastasis survived
for 14 years without treatment of the lung. |
[14] |
1 |
Level 3; Grade D recommendation |
|
Malignant ameloblastoma (metastatic ameloblastoma) in the lung: 3
cases of misdiagnosis as primary lung tumor with a unique growth pattern. |
[15] |
3 |
Level 3; Grade D recommendation |
|
Malignant ameloblastoma: a challenging diagnosis. |
[16] |
1 |
Level 3; Grade D recommendation |
|
Malignant ameloblastoma metastasis to the neck - radiological and
pathohistological dilemma. |
[17] |
1 |
Level 3; Grade D recommendation |
|
Mandible ameloblastoma with lung metastasis: a rare case report. |
[18] |
1 |
Level 3; Grade D recommendation |
|
Metastasizing Ameloblastoma with Localized Interstitial Spread in the
Lung: Report of Two Cases. |
[19] |
2 |
Level 3; Grade D recommendation |
|
Metastasizing Maxillary Ameloblastoma: Report of a Case with Molecular
Characterization. |
[20] |
1 |
Level 3; Grade D recommendation |
|
Multiple Organ Metastases from Ameloblastoma Detected by FDG PET/CT
Imaging. |
[21] |
1 |
Level 3; Grade D recommendation |
|
Pulmonary metastases from an Ameloblastoma: Case report and review of
the literature. |
[22] |
1 |
Level 3; Grade D recommendation |
|
Unicystic ameloblastoma metastasizing to multiple cervical lymph
nodes. |
[23] |
1 |
Level 3; Grade D recommendation |
|
Metastatic ameloblastoma responding to combination chemotherapy: case report
and review of the literature. |
[24] |
1 |
Level 3; Grade D recommendation |
|
Ameloblastoma with varied sites of metastasis: Report of two cases and
literature review. |
[25] |
2 |
Level 3; Grade D recommendation |
|
Metastasizing Ameloblastoma e A perennial pathological enigma? Report
of a case and review of literature. |
[26] |
1 |
Level 3; Grade D recommendation |
|
Review of metastasizing (malignant) ameloblastoma (METAM): pattern of
metastasis and treatment. |
[8] |
1 |
Level 2++; Grade C recommendation |
Regarding to the medical history of the patients, only 2 of the 18 cases admitted to the study provided information: in one patient a history of Alzheimer's disease and advanced stage periodontal disease was recovered, in the second case a positive history was obtained for epithelial cancer and ischaemic heart disease; in no case was a history of toxic habits or infectious diseases such as HPV and EBV reported. In regard to the dental history of the patients admitted to the study, 47.1% reported having received radical surgery in the first or second instance for the maxillofacial tumor diagnosed as ameloblastoma, compared to 52.9% who reported a history of conservative surgery for the same diagnosis. Of the 100% of patients analysed in this study, 44.4% reported a history of recurrent ameloblastoma, while 14.3% reported a history of third molar extraction (Table 3).
Table 3: Clinical-demographic characteristics of published cases of metastasizing
ameloblastoma.
|
Variable |
Number |
Percentage |
|
Sex |
||
|
Man |
9 |
50 |
|
Women |
9 |
50 |
|
Age at tumor diagnosis I |
||
|
< 30 years |
10 |
55.6 |
|
Between 30 - 60 years old |
6 |
33.3 |
|
> 60 years |
2 |
11.1 |
|
Race/Ethnicity |
||
|
Asian Yellow |
14 |
77.8 |
|
Black |
2 |
11.1 |
|
Caucasian |
2 |
11.1 |
|
Medical history |
||
|
Presence of comorbidities |
2 |
100 |
|
Absence of comorbidities |
0 |
0 |
|
Does not report |
16 cases |
|
|
Tumor localization I |
||
|
Jaw |
14 |
77.8 |
|
Maxilla |
4 |
22.2 |
|
Radiographic appearance of tumor I |
||
|
Multilocular radiolucent |
5 |
62.5 |
|
Unilocular radiolucent |
2 |
25 |
|
Diffuse opaque lesion |
1 |
12.5 |
|
Not report |
11 cases |
|
|
Metastasis pattern |
||
|
Distant |
14 |
77.8 |
|
Locoregional |
4 |
22.2 |
|
History of Recurrence |
||
|
Present |
8 |
44.4 |
|
Absent |
10 |
55.6 |
|
Treatment of tumor I |
||
|
Radical surgical |
8 |
47.1 |
|
Conservative surgical |
9 |
52.9 |
|
Not report |
1 case |
|
Given the data obtained with descriptive statistics, we asked ourselves whether clinical parameters such as age at diagnosis of the primary tumor, sex, ethnicity, location and treatment of the initial ameloblastoma influence the metastatic pattern of a MA. To answer this question, we related by contingency table the variable metastatic pattern with the different clinical-demographic parameters indicated. The hypothesis was tested by Pearson's Chi-square test, without obtaining a statistically significant association with any of the variables studied (Table 4). However, it is interesting to note that mandibular location, Asian/yellow and black race, age group under 30 years and conservative surgical approach to the initial tumor showed a higher probability of distant metastasis (Table 4); these data need to be confirmed with a larger sample size. With the results obtained in the initial statistical analysis (Table 4), we asked ourselves whether the age at diagnosis of the primary tumor is a predictor of MA according to gender. To answer this question, we used a contingency table to relate the variable age group according to age at diagnosis of the primary tumor to the variable gender (Table 5). The hypothesis was tested by Pearson's Chi-square test, with a significance level of 0.05. Although the difference was not statistically significant, it could be recognised that the probability of diagnosing an MA is higher when the primary tumor was detected before the age of 30, regardless of gender.
Table 4: Relationship between the pattern of metastasis and clinically important
variables in cases diagnosed as MA.
|
Variable |
Metastasis pattern |
p- value |
||
|
Distant |
Locoregional |
|||
|
Cases (%) |
Cases (%) |
|||
|
Age group according to tumor diagnosis I |
||||
|
< 30 years |
7 (38.9) |
3 (16,6) |
0,1 |
|
|
Between 30 - 60 years old |
6 (33.3) |
0 (0) |
||
|
> 60 years |
1 (5.6) |
1 (5.6) |
||
|
Sex |
Cases (%) |
Cases (%) |
> 0,9 |
|
|
Man |
7 (38.9) |
2 (11.1) |
||
|
Woman |
7 (38.9) |
2 (11.1) |
||
|
Race/ethnicity |
Cases (%) |
Cases (%) |
0,4 |
|
|
Asian yellow |
11 (61) |
3 (16.7) |
||
|
Black |
2 (11.1) |
0 (0) |
||
|
Caucasian |
1 (5.6) |
1 (5.6) |
||
|
Tumor localisation I |
Cases (%) |
Cases (%) |
0,1 |
|
|
Jaw |
10 (55.6) |
4 (22.2) |
||
|
Maxilla |
4 (22.2) |
0 (0) |
||
|
Treatment of tumor I |
Cases (%) |
Cases (%) |
0,5 |
|
|
Radical surgery |
6 (35.3) |
2 (11.7) |
||
|
Conservative surgery |
8 (47,1) |
1 (5.9) |
||
Table 5: Analysis of association between clinically important variables in MA
with age at diagnosis of the primary tumor.
|
Clinical/demographic
aspects |
Age category |
|
||
|
< 30 years |
30 -60 years |
> 60 years |
p-value |
|
|
No. of cases (%) |
No. of cases (%) |
No. of cases (%) |
||
|
Sex |
|
|
|
0,2 |
|
Female |
5 (27.8) |
4 (22.2) |
0 (0) |
|
|
Male |
5 (27.8) |
2 (11.1) |
2 (11.1) |
|
Note: The probability of occurrence of an MA is
slightly higher when the diagnosis of the primary tumor occurs before the age
of 30, irrespective of gender or sex.
II Pathological Features Associated with MA
Of the total number of patients admitted to the study (N=18), the clinicopathological variant was reported in only 15 cases, with the conventional (solid/multicystic) type of ameloblastoma predominating in the series analysed. Less than 15% of the reported cases corresponded to the unicystic variant (Table 6). Regarding the histopathological sub-variant of the primary tumor, only 13 cases provided this data, with a higher representation of the follicular subtype, with almost half of the documented clinical cases, followed by the plexiform subtype. Only one case was reported as acanthomatous AM, only one case as intraluminal and only one case as mixed (follicular/plexiform) ameloblastoma (Table 6). None of the articles processed (N=14) provided information on the surgical margins of the primary tumor. Based on the data obtained by descriptive statistics, we asked ourselves whether there was an association between the metastatic pattern and the pathology of the primary tumor; to answer both questions we performed a categorical analysis by contingency table and Chi-square test. The statistical analysis did not allow us to recognise a significant association between the variables studied; however, it is worth noting the greater probability of occurrence of an MA with a distant pattern given a primary tumor with a conventional variant (solid/multicystic) and follicular growth subtype (Table 7).
Table 6: Pathological features of published cases of metastasizing ameloblastoma.
|
Variable |
Number |
Percentage |
|
Clinicopathological variant |
||
|
Conventional |
13 |
86.7 |
|
Unicystic |
2 |
13.3 |
|
Not report |
3 cases |
|
|
Histological subtype |
||
|
Follicular |
6 |
46.2 |
|
Plexiform |
4 |
30.8 |
|
Other |
3 |
|
|
Not report |
5 cases |
|
Table 7: Relationship between the pattern of metastasis and pathologically
important variables in cases diagnosed as MA and recovered in this study.
|
Variable |
Metastasis pattern |
p- value |
||
|
Distant |
Locoregional |
|||
|
Cases (%) |
Cases (%) |
|||
|
Clinicopathological variant |
||||
|
Conventional |
11 (73.3) |
2 (13.3) |
0,3 |
|
|
Unicystic |
1 (6.7) |
1 (6.7) |
||
|
Histological subtype |
Cases (%) |
Cases (%) |
||
|
Follicular |
5 (38.5) |
1 (7,7) |
0,3 |
|
|
Other |
4 (30.8) |
3 (23) |
||
Note: None of the pathological parameters
analysed showed significant association with the metastatic pattern of
ameloblastoma. However, it is likely that by increasing the "N" we
can more accurately assess the relationship between metastatic pattern and
histological subtype.
III Molecular Characteristics Associated with MA
Of the 18 clinical cases retrieved from the total number of articles selected, only 11 cases reported information on the molecular profile of the primary tumor, with wide heterogeneity of data and markers investigated. Table 8 shows that less than 10% of the reported MA cases had a molecular profile of the primary tumor positive exclusively for MAPK pathway genes such as BRAF. In 81% of the published cases, positivity was recovered for genes other than those comprising the MAPK pathway such as EGFR, p53, Ki67, Cytokeratins, EMA, TIF-1, HER2, p63, Wapsin A and PCK; in one case (9.1%) positivity was reported for both MAPK and BRAF and non-MAPK genes (Table 8).
Table 8: Molecular characteristics in cases diagnosed and published as MA.
|
Variable |
No. of cases |
Percentage |
|
MAPK genes |
1 |
9.1 |
|
Non-MAPK genes |
9 |
81.8 |
|
Both markers |
1 |
9.1 |
|
Uninformed |
||
Note: Of the 18 clinical cases entered into the
study, 7 cases did not report the molecular profile of the primary tumor.
Given the results obtained in the descriptive statistics, we wondered whether a particular molecular profile could explain the pattern of metastasis in cases of ameloblastoma with this form of clinical presentation. To answer this question, we performed a categorical analysis by contingency table and Chi-square test, obtaining that the molecular profile does not affect the metastatic pattern of an ameloblastoma with this potential (Table 9). However, it is necessary to confirm these results with a larger number of clinical cases; additionally, it is necessary that each case of MA diagnosed is published with the molecular profile looking for MAPK pathway genes and non-MAPK genes that have shown association with ameloblastoma and its prognosis such as SMO, p53-MM2, metalloproteases, NOTCH pathway, Ki67, and genes that promote epithelial mesenchymal transition such as SLUG, TGF-B, E-cadherin and Syndecan-1 [6, 9, 10]. None of the published cases investigated, from a molecular point of view, the presence of cells with stem cell phenotype in the pathology of the primary tumor; an aspect that we consider important, as recent research has detected in ameloblastomas a subpopulation of epithelial cells with stem-like characteristics, classified as AM-EpiSCs LGR5+ [10].
Table 9: Association by categorical analysis of the molecular profile of the
primary tumor in reported cases of MA with the reported metastatic pattern.
|
Metastasis pattern |
Molecular profile of tumor I |
p- value |
||
|
MAPK genes (%) |
Non-MAPK genes (%) |
Both markers (%) |
||
|
Distant |
1 (9.1) |
7 (63.6) |
0 (0) |
0.2 |
|
Locoregional |
0 (0) |
2 (18.2) |
1 (9.1) |
|
Note: Categorical analysis demonstrates no
significant association between the molecular profile of the primary tumor and
the metastatic pattern in patients with this diagnosis.
Discussion
In 2011, thanks to the emblematic work of Hanahan and Weinberg, the phenotypes that characterise a malignant cell became known, one of them being the capacity to metastasise locally or at a distance [27]. This means that metastasis is cancer; however, the latest edition of the WHO on odontogenic tumors classified MA as a benign variant of ameloblastoma, and despite this, the prognosis of this pathological entity is not encouraging [6, 7]. In view of this, we set out to determine by systematic review of clinical case reports published in the last 10 years, the association between clinicopathological and/or molecular factors and metastasizing ameloblastoma with a view to understanding its pathogenesis, and to find possible predictors for this clinical entity with contradictory histology.
MA is a tumor of rare occurrence, with less than 1% incidence, being diagnosed as metastatic at the time of the primary lesion in 15% of cases, while in a high proportion this variant of ameloblastoma is diagnosed between 3 months to 24 years after the primary tumor, with an average latency time of 8.23 years [7]. The underlying mechanisms that would lead a benign tumor such as AM to metastasise are not fully understood; based on data from benign tumors of similar behaviour such as metastasising pleomorphic adenoma or benign fibrous cutaneous metastasising histiocytoma, it is hypothesised that incomplete removal of the primary tumor or a history of multiple surgical interventions for recurrent tumor favour haematogenous spread of tumor cells with consequent metastasis [28-31]. However, some do not accept this theory, given the ability of the immune system to inactivate tumor cells present in the bloodstream by cell-mediated immune-dependent mechanisms [7, 32, 33]. Praetorius in his 2009 review on malignant odontogenic tumors proposes the size and evolution of the primary tumor, mandibular location, repeated and incomplete surgical interventions, or a primary tumor treated with chemotherapy and radiotherapy, as possible clinical predictors of metastasis [34]. However, the underlying mechanism by which each of these factors influences the pathogenesis of MA remains to be elucidated.
In our series, MA showed no gender predilection, with a male to female ratio of 1:1. This finding is in agreement with the report of Luo et al.; although, other studies have reported a subtle male predominance of MA [7, 8, 22, 35]. The mean age at diagnosis of MA was 46 years, which is very close to that reported by Deepak et al. in their review, where the mean age was 42.62 years, and another study by Dissanayake et al. reported a mean age of 33.85 years [8, 35]. When analysing the relationship between the age at diagnosis of the initial ameloblastoma or primary tumor and the appearance of metastases according to sex, we found that the possibility of diagnosing a metastatic ameloblastoma is 1.3 times higher when the primary tumor was detected before the age of 30 years, with no differences with respect to sex (Table 5), although the difference was not statistically significant, which may be due to a low sample size.
Regarding the clinical characteristics of the primary tumor in our series, 77.8% of the diagnosed metastasizing ameloblastomas had their primary located in the mandible, with a mandible/maxilla ratio of 4:1 (Table 4), coinciding with other reports that place the lower jaw as the site most involved by ameloblastoma [8, 23, 36]. In fact, previous evidence suggests that the mandible is a possible predictor of MA [34]. In reference to the location of metastasis, the distant metastatic pattern accounted for 78.6% of the cases analysed (Table 3), with the lung being the site of greatest involvement, which is consistent with other reports [7, 17, 35]. When relating the pattern of metastasis to the different eligible clinical-demographic variables, although no statistically significant association was obtained, markers such as mandibular location, early diagnosis of a primary AM, and yellow Asian race are associated with a higher probability of distant metastasis as a clinical presentation of an MA (Table 4). No reports were found that have analysed this association to contrast our results, but with respect to ethnicity/race, Ikemura et al., in their report on 15 confirmed cases of metastatic ameloblastoma, 8 of them were Japanese cases, and the authors highlighted the preponderance of this diagnosis in this racial group, also indicating that Japan exhibits a higher incidence of ameloblastoma than Western countries [37].
Histologically, in both the primary tumor and metastasis, the conventional variant (solid/multicystic) was the most prevalent in our series (Table 5), coinciding with the findings of Pandiar et al., and the WHO consensus [1, 35]. With respect to histological subtype, previous evidence indicates that the plexiform or mixed (follicular/plexiform) variant commonly exhibits a higher likelihood of metastasis [33]. However, in our series the most prevalent histological subtype was follicular, accounting for 46.2% of cases, followed by the plexiform subtype with 30.8% representation (Table 6). These data coincide with the findings of Pandiar et al., and Ikemura et al., fact, Ikemura's group published in 1972 that, after evaluating 14 cases of metastatic ameloblastoma, 50% of the primary tumors presented the follicular type of growth [35, 37]. According to Pandiar and his group, the follicular variant histologically follows a growth pattern reminiscent of odontogenesis prior to morpho differentiation, with abundant bud-like structures [35]. They postulate that during surgical procedures these structures may detach and implant elsewhere, but other authors such as Kunze et al. dismiss this theory [33, 35].
With respect to the treatment scheme with which the primary tumor was approached, 53% of our series received a conservative surgical approach in the management of their initial AM, with a 1.1:1 ratio with respect to metastatic ameloblastomas with a history of radical surgery (Table 3). When we related the primary tumor treatment variable to the pattern of dissemination, we found that those metastatic tumors with a history of conservative surgical approach based on curettage of their primary tumor were more likely to have distant metastases, although the difference was not statistically significant (Table 4). It is possible that during surgery, even if it is radical and the first treatment option for conventional intraosseous ameloblastoma, tumor cells with a stem phenotype may be aspirated, causing seeding and generation of foci in other sites such as the lung [38]. Indeed, Vorzimer and Perla reported the presence of tumor cylinders in the lumen of the bronchi of a patient with pulmonary metastasis of an ameloblastoma in only one case published to date [39]. The route of dissemination of tumor cells in an AM is not entirely clear, according to Laughlin the main route of dissemination in an AM would be the haematogenous route, given the reported cases of MA in different sites such as bone, liver, brain, skin, as well as lung and lymph nodes [40].
According to Laughlin, one of the reasons why a benign slow-growing tumor such as ameloblastoma might demonstrate a metastatic phenotype is its recurrent behavior, favoured by incomplete and inadequate removal of the primary tumor by curettage, radiotherapy and chemotherapy [40]. In our study, less than half of the cases of MA had a history of recurrence (Table 3), which is consistent with the results of Hosalkar et al. in their study, about a quarter of the cases of MA had a history of recurrence [7]. When we related the pattern of metastasis to the history of recurrence in MA, we did not obtain a statistically significant association, implying that recurrence cannot be considered a predictor of metastasis in ameloblastoma. This conclusion is supported by several clinical case reports on metastatic ameloblastoma without a history of recurrence [8, 15, 17, 23-26].
Regarding the molecular characteristics associated with MA, 81.8% of the metastatic tumors had a history of primary tumor positivity for non-MAPK pathway genes (Table 8), some of them such as p63 and high expression for Ki67. This is similar to a review by Anjali et al. in which about 5 cases of MA report positivity for these genes [41]. When relating the molecular profile of the primary tumor to the pattern of metastasis, it was found that the probability of diagnosing an ameloblastoma with distant metastasis is higher if its primary tumor associated positivity for non-MAPK genes (Table 9), although the difference was not statistically significant, most likely a result of the low number of reported cases. No studies with this type of analysis were found to contrast our results.
The weaknesses of our study are based on limited evidence regarding the clinical history of each case, as well as scarce or poor information on the primary lesion, its detailed radiographic appearance and its size. Likewise, with regard to the molecular characteristics, the lack of homogeneity between the different cases does not allow us to create a pattern of association between the different genes and the probability of metastasis of an ameloblastoma. In view of these limitations, we suggest that every case published on MA should contain a complete medical and odontostomatological history, with emphasis on the search for comorbidities, toxic, sexual and dietary habits, and a history of periodontal disease, as several studies have proposed smoked and chewed tobacco, chronic alcohol consumption, viral and fungal infections and chronic periodontitis as risk factors for oral cancer, in addition, another clinical factor that has been shown to be a key factor in carcinogenesis is obesity, and we therefore recommend that the body mass index of each patient should be reported in every case published on MA, as the pathogenic mechanism by which obesity may promote the progression of a malignant tumor has recently been published [42-46]. For all these reasons, we believe that a complete anamnesis could provide us with additional data of importance in the prognosis of an ameloblastoma; additionally, a detailed description of the primary lesion in terms of size and radiographic features, as well as homogeneity in terms of molecular markers will provide us with a better scenario for predicting the biological behaviour of an AM; and with respect to the molecular profile of this tumor, we recommend that every published case of MA should report the association with MAPK genes (RAS, BRAF, FGFR2), and non-MAPK genes such as SMO, p53, Ki67, p63, plus markers of epithelial-mesenchymal transition and stem phenotype cells such as AM-EpiSCs/LGR5+. This since molecular biology studies have recognised two different genetic pathways exacerbated in ameloblastomas, as 90% of these tumors show mutations in genes of the MAPK (mitogen-activated protein kinase) pathway, of which the BRAF oncogene has been recognised as activated in 63% of ameloblastomas as a product of a point mutation V600E (change of valine to glutamate at codon 600); while 16-39% of ameloblastomas associate activating mutations in non-MAPK pathway genes (Hedgehog and WNT/beta-catenin pathways) such as SMO (G protein-coupled receptor and effector signalling component of the SHH pathway) [6, 8, 9]. The causes that would lead to the activation of these oncogenes are not fully understood; limited evidence from descriptive studies based on molecular pathology demonstrates the possible involvement of tobacco, viruses such as HPV and EBV in the aetiopathogenesis of AM, and recently a subpopulation of epithelial cells with the ability to co-express the LGR5 marker and stem phenotype genes was reported in samples of solid ameloblastomas with follicular, mixed and desmoplastic subvariants, termed AM-EpiSCs LGR5+ [47-50]. The LGR5 marker is a G protein-coupled receptor with leucine-rich repeats, a member of the LGR family of proteins, and has been identified as a marker of stem cells as well as cancer stem cells (CSCs) in several cancer types.
Functionally, LGR5 has been shown to promote epithelial-mesenchymal transition in hepatocellular carcinoma, colon cancer and glioma, and is associated with poor survival in glioma patients. This subpopulation of AM-SCs-LGR5+ cells have been shown to be functionally more adept at forming 3D spheroids and 3D human tumor organoids, which reproduced the histopathological features of different subtypes of solid ameloblastoma. Additionally, in vitro resistance of these cells to the BRAFV600E inhibitor (vemurafenib) has been reported, playing a key role in the pathogenesis and recurrence of AM [10]. Based on this background, we consider it necessary to investigate this cell subtype in the pathophysiology of metastasizing ameloblastoma.
Conclusion
MA is a very rare pathology that has been, surprisingly, reclassified as benign in the latest WHO consensus of 2017 for odontogenic tumors. Its diagnosis is approached in a retrospective manner on primary AM and its prediction is, for the moment, impossible given the scarcity of homogeneity in the clinical cases published on the MA entity, with respect to clinical, pathological and molecular criteria. Regarding the latter, there is a wide heterogeneity in the markers studied. Based on the results obtained in the present study, it is likely that an early initial diagnosis (< 30 years) of AM, yellow Asian race, mandibular location, conventional variant (solid/multicystic), and follicular subtype of growth are possible predictors of metastatic behaviour in benign slow-growing tumors such as AM. Our findings also lead us to doubt the predictive potential that has been assigned to factors such as history of recurrence and type of surgical approach in the primary tumor or initial AM. Regarding the molecular profile as a candidate predictor of MA, we have no literature to support our findings, therefore, the possible impact of non-MAPK genes in the pathogenesis of MA is inconclusive. Further studies with a full clinicopathological report are needed to corroborate our findings.
Conflicts of Interest
None.
Acknowledgement
We are thankful to our patients for giving us the opportunity to learn.
Article Info
Article Type
Review of LiteraturePublication history
Received: Tue 01, Jun 2021Accepted: Sat 12, Jun 2021
Published: Thu 01, Jul 2021
Copyright
© 2023 Juan Fernando Buestan Zambrano. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.DOBCR.2021.03.01
Figures & Tables
Table 1: Summary of the total number of studies obtained and filtered by
scientific database used in the study.
|
DATABASE |
Total publications |
Excluded by language |
Not relevant |
Incomplete text |
Total including |
|
PubMed |
82 |
0 |
55 |
16 |
11 |
|
ScienceDirect |
275 |
0 |
267 |
4 |
3 |
|
Cochrane |
7 |
0 |
7 |
0 |
0 |
Table 2: List of studies with their respective clinical cases reported and
selected under the inclusion criteria established in this review.
|
Study |
Reference Number |
Number of clinical cases reported |
Level of evidence and recommendation according to SIGN [13] |
|
A case of ameloblastoma with extensive pulmonary metastasis survived
for 14 years without treatment of the lung. |
[14] |
1 |
Level 3; Grade D recommendation |
|
Malignant ameloblastoma (metastatic ameloblastoma) in the lung: 3
cases of misdiagnosis as primary lung tumor with a unique growth pattern. |
[15] |
3 |
Level 3; Grade D recommendation |
|
Malignant ameloblastoma: a challenging diagnosis. |
[16] |
1 |
Level 3; Grade D recommendation |
|
Malignant ameloblastoma metastasis to the neck - radiological and
pathohistological dilemma. |
[17] |
1 |
Level 3; Grade D recommendation |
|
Mandible ameloblastoma with lung metastasis: a rare case report. |
[18] |
1 |
Level 3; Grade D recommendation |
|
Metastasizing Ameloblastoma with Localized Interstitial Spread in the
Lung: Report of Two Cases. |
[19] |
2 |
Level 3; Grade D recommendation |
|
Metastasizing Maxillary Ameloblastoma: Report of a Case with Molecular
Characterization. |
[20] |
1 |
Level 3; Grade D recommendation |
|
Multiple Organ Metastases from Ameloblastoma Detected by FDG PET/CT
Imaging. |
[21] |
1 |
Level 3; Grade D recommendation |
|
Pulmonary metastases from an Ameloblastoma: Case report and review of
the literature. |
[22] |
1 |
Level 3; Grade D recommendation |
|
Unicystic ameloblastoma metastasizing to multiple cervical lymph
nodes. |
[23] |
1 |
Level 3; Grade D recommendation |
|
Metastatic ameloblastoma responding to combination chemotherapy: case report
and review of the literature. |
[24] |
1 |
Level 3; Grade D recommendation |
|
Ameloblastoma with varied sites of metastasis: Report of two cases and
literature review. |
[25] |
2 |
Level 3; Grade D recommendation |
|
Metastasizing Ameloblastoma e A perennial pathological enigma? Report
of a case and review of literature. |
[26] |
1 |
Level 3; Grade D recommendation |
|
Review of metastasizing (malignant) ameloblastoma (METAM): pattern of
metastasis and treatment. |
[8] |
1 |
Level 2++; Grade C recommendation |
Table 3: Clinical-demographic characteristics of published cases of metastasizing
ameloblastoma.
|
Variable |
Number |
Percentage |
|
Sex |
||
|
Man |
9 |
50 |
|
Women |
9 |
50 |
|
Age at tumor diagnosis I |
||
|
< 30 years |
10 |
55.6 |
|
Between 30 - 60 years old |
6 |
33.3 |
|
> 60 years |
2 |
11.1 |
|
Race/Ethnicity |
||
|
Asian Yellow |
14 |
77.8 |
|
Black |
2 |
11.1 |
|
Caucasian |
2 |
11.1 |
|
Medical history |
||
|
Presence of comorbidities |
2 |
100 |
|
Absence of comorbidities |
0 |
0 |
|
Does not report |
16 cases |
|
|
Tumor localization I |
||
|
Jaw |
14 |
77.8 |
|
Maxilla |
4 |
22.2 |
|
Radiographic appearance of tumor I |
||
|
Multilocular radiolucent |
5 |
62.5 |
|
Unilocular radiolucent |
2 |
25 |
|
Diffuse opaque lesion |
1 |
12.5 |
|
Not report |
11 cases |
|
|
Metastasis pattern |
||
|
Distant |
14 |
77.8 |
|
Locoregional |
4 |
22.2 |
|
History of Recurrence |
||
|
Present |
8 |
44.4 |
|
Absent |
10 |
55.6 |
|
Treatment of tumor I |
||
|
Radical surgical |
8 |
47.1 |
|
Conservative surgical |
9 |
52.9 |
|
Not report |
1 case |
|
Table 4: Relationship between the pattern of metastasis and clinically important
variables in cases diagnosed as MA.
|
Variable |
Metastasis pattern |
p- value |
||
|
Distant |
Locoregional |
|||
|
Cases (%) |
Cases (%) |
|||
|
Age group according to tumor diagnosis I |
||||
|
< 30 years |
7 (38.9) |
3 (16,6) |
0,1 |
|
|
Between 30 - 60 years old |
6 (33.3) |
0 (0) |
||
|
> 60 years |
1 (5.6) |
1 (5.6) |
||
|
Sex |
Cases (%) |
Cases (%) |
> 0,9 |
|
|
Man |
7 (38.9) |
2 (11.1) |
||
|
Woman |
7 (38.9) |
2 (11.1) |
||
|
Race/ethnicity |
Cases (%) |
Cases (%) |
0,4 |
|
|
Asian yellow |
11 (61) |
3 (16.7) |
||
|
Black |
2 (11.1) |
0 (0) |
||
|
Caucasian |
1 (5.6) |
1 (5.6) |
||
|
Tumor localisation I |
Cases (%) |
Cases (%) |
0,1 |
|
|
Jaw |
10 (55.6) |
4 (22.2) |
||
|
Maxilla |
4 (22.2) |
0 (0) |
||
|
Treatment of tumor I |
Cases (%) |
Cases (%) |
0,5 |
|
|
Radical surgery |
6 (35.3) |
2 (11.7) |
||
|
Conservative surgery |
8 (47,1) |
1 (5.9) |
||
Table 5: Analysis of association between clinically important variables in MA
with age at diagnosis of the primary tumor.
|
Clinical/demographic
aspects |
Age category |
|
||
|
< 30 years |
30 -60 years |
> 60 years |
p-value |
|
|
No. of cases (%) |
No. of cases (%) |
No. of cases (%) |
||
|
Sex |
|
|
|
0,2 |
|
Female |
5 (27.8) |
4 (22.2) |
0 (0) |
|
|
Male |
5 (27.8) |
2 (11.1) |
2 (11.1) |
|
Note: The probability of occurrence of an MA is
slightly higher when the diagnosis of the primary tumor occurs before the age
of 30, irrespective of gender or sex.
Table 6: Pathological features of published cases of metastasizing ameloblastoma.
|
Variable |
Number |
Percentage |
|
Clinicopathological variant |
||
|
Conventional |
13 |
86.7 |
|
Unicystic |
2 |
13.3 |
|
Not report |
3 cases |
|
|
Histological subtype |
||
|
Follicular |
6 |
46.2 |
|
Plexiform |
4 |
30.8 |
|
Other |
3 |
|
|
Not report |
5 cases |
|
Table 7: Relationship between the pattern of metastasis and pathologically
important variables in cases diagnosed as MA and recovered in this study.
|
Variable |
Metastasis pattern |
p- value |
||
|
Distant |
Locoregional |
|||
|
Cases (%) |
Cases (%) |
|||
|
Clinicopathological variant |
||||
|
Conventional |
11 (73.3) |
2 (13.3) |
0,3 |
|
|
Unicystic |
1 (6.7) |
1 (6.7) |
||
|
Histological subtype |
Cases (%) |
Cases (%) |
||
|
Follicular |
5 (38.5) |
1 (7,7) |
0,3 |
|
|
Other |
4 (30.8) |
3 (23) |
||
Note: None of the pathological parameters
analysed showed significant association with the metastatic pattern of
ameloblastoma. However, it is likely that by increasing the "N" we
can more accurately assess the relationship between metastatic pattern and
histological subtype.
Table 8: Molecular characteristics in cases diagnosed and published as MA.
|
Variable |
No. of cases |
Percentage |
|
MAPK genes |
1 |
9.1 |
|
Non-MAPK genes |
9 |
81.8 |
|
Both markers |
1 |
9.1 |
|
Uninformed |
||
Note: Of the 18 clinical cases entered into the
study, 7 cases did not report the molecular profile of the primary tumor.
Table 9: Association by categorical analysis of the molecular profile of the
primary tumor in reported cases of MA with the reported metastatic pattern.
|
Metastasis pattern |
Molecular profile of tumor I |
p- value |
||
|
MAPK genes (%) |
Non-MAPK genes (%) |
Both markers (%) |
||
|
Distant |
1 (9.1) |
7 (63.6) |
0 (0) |
0.2 |
|
Locoregional |
0 (0) |
2 (18.2) |
1 (9.1) |
|
Note: Categorical analysis demonstrates no
significant association between the molecular profile of the primary tumor and
the metastatic pattern in patients with this diagnosis.
References
1.
El Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg
PJ (2017) WHO Classification of Head and
Neck Tumours. Int Agency Res Cancer 9.
2.
Small IA, Waldron
CA (1955) Ameloblastomas of the jaws. Oral Surg Oral Med Oral Pathol 8:
281-297. [Crossref]
3.
Hong J, Yun PY,
Chung IH, Myoung H, Suh JD et al. (2007) Long-term follow up on recurrence of
305 ameloblastoma cases. Int J Oral Maxillofac Surg 36: 283-288. [Crossref]
4. Córdova Alvarez MJ,
Benenaula Bojorque JA (2017) Prevalencia de tumores benignos de origen odontogénico
en pacientes atendidos en el Hospital Eugenio Espejo durante los años 2011 a
2016. Univ Central Del Ecuador.
5. De Medeiros WKD, da
Silva LP, Santos PPA, Pinto LP, de Souza LB (2018) Clinicopathological analysis of odontogenic tumors
over 22 years period: Experience of a single center in northeastern Brazil. Med Oral Patol Oral
Cir Bucal 23: e664-e671. [Crossref]
6.
Soluk Tekkeşin M,
Wright JM (2018) The World Health Organization Classification of Odontogenic
Lesions: A Summary of the Changes of the 2017 (4th) Edition. Turk Patoloji
Derg 34. [Crossref]
7.
Hosalkar R,
Saluja TS, Swain N, Singh SK (2021) Prognostic evaluation of metastasizing
ameloblastoma: A systematic review of reported cases in literature. J
Stomatol Oral Maxillofac Surg 122: 192-198. [Crossref]
8.
Dissanayake RKG,
Jayasooriya PR, Siriwardena DJL, Tilakaratne WM (2011) Review of metastasizing
(malignant) ameloblastoma (METAM): pattern of metastasis and treatment. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod 111: 734-741. [Crossref]
9.
Abdel Aziz A, Amin MM (2012) EGFR, CD10 and proliferation marker Ki67 expression in
ameloblastoma: possible role in local recurrence. Diagn Pathol 7: 14. [Crossref]
10.
Brown NA, Betz BL
(2015) Ameloblastoma: A Review of Recent Molecular Pathogenetic Discoveries. Biomark
Cancer 7: 19-24. [Crossref]
11. Moher D, Liberati A, Tetzlaff J, Altman DG, Altman D
et al. (2009) Preferred reporting items for systematic reviews and
meta-analyses: The PRISMA statement. PLoS Med 6: e1000097. [Crossref]
12.
Pinillo León AL, Cañedo Andalia R (2005) El MeSH: Una
herramienta clave para la búsqueda de información en la base de datos Medline. Acimed 13.
13.
Petrisor BA,
Keating J, Schemitsch E (2006) Grading the evidence: levels of evidence and
grades of recommendation. Injury 37: 321-327. [Crossref]
14.
Ikai A, Suzuki S,
Hayashi K (2016) A case of ameloblastoma with extensive pulmonary metastasis
survived for 14 years without treatment of the lung. J Oral Maxillofac Surg
Med Pathol 28: 138-142.
15.
Bi R, Shen L, Zhu
X, Xu X (2015) Malignant ameloblastoma (metastatic ameloblastoma) in the lung:
3 cases of misdiagnosis as primary lung tumor with a unique growth pattern. Diagn
Pathol 10: 123. [Crossref]
16.
Salami A, Ezenkwa
U, Salami M, Ajani M, Okolo C (2018) Malignant ameloblastoma: a challenging
diagnosis. Autops Case Rep 8: e2018043. [Crossref]
17. Golubović M, Petrović M, Jelovac DB, Nenezić DU,
Antunović M (2012) Metastaza malignog ameloblastoma na vratu-radiološka i patohistološka
dilema. Vojnosanit Pregl 69: 444-448.
18.
Yang RN, Wang XS,
Ren J, Xie YF, Zhou D et al. (2015) Mandible ameloblastoma with lung
metastasis: a rare case report. Int J Clin Exp Pathol 8: 6793-6799. [Crossref]
19.
Chou YH, Jhuang
JY, Chang MH, Huang WC, Hsieh MS (2014) Metastasizing Ameloblastoma With
Localized Interstitial Spread in the Lung: Report of Two Cases. Int J Surg
Pathol 22: 343-346. [Crossref]
20.
Rotellini M,
Maggiore G, Trovati M, Saraceno MS, Franchi A (2016) Metastasizing Maxillary
Ameloblastoma: Report of a Case with Molecular Characterization. J Oral
Maxillofac Res 7: e5. [Crossref]
21.
Niu N, Chen L,
Liu Y, Li F (2013) Multiple organ metastases from ameloblastoma detected by FDG
PET/CT imaging. Clin Nucl Med 38: 1009-1011. [Crossref]
22.
Luo DY, Feng CJ,
Guo JB (2012) Pulmonary metastases from an Ameloblastoma: case report and
review of the literature. J Craniomaxillofac Surg 40: e470-e474. [Crossref]
23.
Noguchi K, Kishimoto H, Yamanegi K, Moridera K,
Takaoka K et al. (2013) Unicystic
ameloblastoma metastasizing to multiple cervical lymph nodes. J Surg Case
Rep 2013: rjt033. [Crossref]
24.
Amzerin M,
Fadoukhair Z, Belbaraka R, Iraqui M, Boutayeb S et al. (2011) Metastatic
ameloblastoma responding to combination chemotherapy: case report and review of
the literature. J Med Case Rep 5: 491. [Crossref]
25.
Lin Y, He JF, Li
ZY, Liu JH (2014) Ameloblastoma with varied sites of metastasis: report of two
cases and literature review. J Craniomaxillofac Surg 42: e301-e304. [Crossref]
26.
Jayaraj G,
Sherlin HJ, Ramani P, Premkumar P, Natesan A et al. (2014) Metastasizing
Ameloblastoma - a perennial pathological enigma? Report of a case and review of
literature. J Craniomaxillofac Surg 42: 772-779. [Crossref]
27.
Hanahan D,
Weinberg RA (2011) Hallmarks of cancer: the next generation. Cell 144:
646-674. [Crossref]
28.
Patton KT, Cheng L, Papavero V, Blum MG, Yeldandi AV et
al. (2006) Benign metastasizing
leiomyoma: clonality, telomere length and clinicopathologic analysis. Mod
Pathol 19: 130-140. [Crossref]
29.
Knight J,
Ratnasingham K (2015) Metastasising pleomorphic adenoma: Systematic review. Int
J Surg 19: 137-145. [Crossref]
30.
Doyle LA,
Fletcher CDM (2013) Metastasizing “benign” cutaneous fibrous histiocytoma: a
clinicopathologic analysis of 16 cases. Am J Surg Pathol 37: 484-495. [Crossref]
31.
Barnaś E, Raś R,
Skręt Magierło J, Wesecki M, Filipowska J et al. (2019) Natural history of
leiomyomas beyond the uterus. Medicine 98: e15877. [Crossref]
32.
Houston G,
Davenport W, Keaton W, Harris S (1993) Malignant (metastatic) ameloblastoma:
report of a case. J Oral Maxillofac Surg 51: 1152-1155. [Crossref]
33.
Kunze E, Donath
K, Luhr HG, Engelhardt W, De Vivie R (1985) Biology of metastasizing
ameloblastoma. Pathol Res Pract 180: 526-535. [Crossref]
34.
Praetorius F
(2017) Malignant odontogenic tumours. Surg Pathol head neck odontogenic tumours.
New York: Informa Healthcare 12902.
35.
Pandiar D, Anand
R, Kamboj M, Narwal A, Shameena PM et al. (2021) Metastasizing Ameloblastoma: A
10 Year Clinicopathological Review with an Insight Into Pathogenesis. Head
Neck Pathol. [Crossref]
36.
Van Dam SD, Unni
KK, Keller EE (2010) Metastasizing (malignant) ameloblastoma: review of a
unique histopathologic entity and report of Mayo Clinic experience. J Oral
Maxillofac Surg 68: 2962-2974. [Crossref]
37.
Ikemura K,
Tashiro H, Fujino H, Ohbu D, Nakajima K (1972) Ameloblastoma of the mandible
with metastasis to the lungs and lymph nodes. Cancer 29: 930-940. [Crossref]
38. Effiom OA, Ogundana OM, Akinshipo AO, Akintoye SO
(2018) Ameloblastoma: current etiopathological concepts and management. Oral Dis 24: 307-316. [Crossref]
39.
Vorzimer J, Perla D (1932) An Instance of Adamantinoma of the Jaw with Metastases
to the Right Lung. Am J Pathol 8: 445-454.3. [Crossref]
40.
Laughlin EH
(1989) Metastasizing ameloblastoma. Cancer 64: 776-780. [Crossref]
41.
Ganjre AP, Sarode
G, Sarode S (2019) Molecular characterization of metastasizing ameloblastoma: A
comprehensive review. J Cancer Res Ther 15: 455-462. [Crossref]
42.
Sanjaya PR, Gokul S, Gururaj Patil B, Raju R (2011) Candida in oral pre-cancer and oral cancer. Med
Hypotheses 77: 1125-1128. [Crossref]
43.
Hübbers CU, Akgül
B (2015) HPV and cancer of the oral cavity. Virulence 6: 244-248. [Crossref]
44.
Rischin D, Ferris
RL, Le QT (2015) Overview of Advances in Head and Neck Cancer. J Clin Oncol
33: 3225-3226. [Crossref]
45.
Shaikh MH,
McMillan NAJ, Johnson NW (2015) HPV-associated head and neck cancers in the
Asia Pacific: A critical literature review & meta-analysis. Cancer
Epidemiol 39: 923-938. [Crossref]
46.
Benaiges E, Ceperuelo Mallafré V, Madeira A, Bosch R,
Núñez Roa C et al. (2021) Survivin drives
tumor-associated macrophage reprogramming: a novel mechanism with potential
impact for obesity. Cell Oncol. [Crossref]
47.
Guan P, Wong SF,
Lim JQ, Ng CCY, Soong PL et al. (2019) Mutational Signatures in Mandibular
Ameloblastoma Correlate with Smoking. J Dent Res 98: 652-658. [Crossref]
48.
Namin AK, Azad
TM, Eslami B, Sarkarat F, Shahrokhi M et al. (2003) A study of the relationship
between ameloblastoma and human papilloma virus. J Oral Maxillofac Surg
61: 467-470. [Crossref]
49. Kahn MA (1989) Ameloblastoma in young persons: a clinicopathologic analysis and etiologic investigation. Oral Surg Oral Med Oral Pathol 67: 706-715. [Crossref]
50. Fujita S, Shibata Y, Takahashi H, Tsuda N, Okabe H (1997) Latent infection with Epstein-Barr virus in odontogenic disorders: comparison among ameloblastoma, dentigerous cyst and odontogenic keratocyst. Pathol Int 47: 449-453. [Crossref]