Journals
Minimally invasive operation for costal arch deformity
A B S T R A C T
Costal arch deformity is one of the thoracic deformities, but it was always regarded as a part of other complex deformities. The former surgical methods for this deformity are only affiliated procedures, which are not suitable for independent costal arch deformity. We encountered a large number of patients with single rib arch malformation in our clinical practice. In order to treat this special kind of deformity, we designed a minimally invasive procedure.
K E Y W O R D S
Costal arch deformity, minimally invasive, operation
Introduction
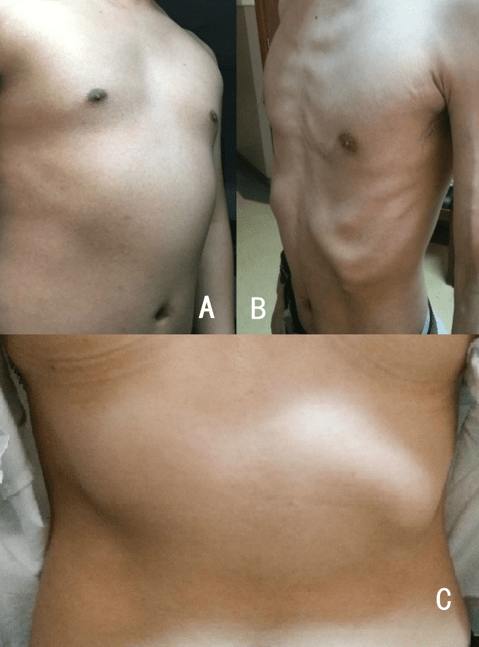
In all kinds of thoracic deformities, pectus excavatum and puctus carinatum are the relatively more common kinds [1]. Other deformities are rarely mentioned, and costal arch deformity is one of them. This deformity exists at both sides of the rib arch and can be of different shapes (Fig 1), but it is always considered to be a part of other complex malformations, so it has been only treated by an affiliated operation by some surgeons [2, 3]. In the early Ravitch surgery, the method was to remove the local costal cartilages and connect the remaining rib arch with the sternum [1]. In 2016, Park and colleagues [2] proposed an additional "magic string" technique to correct the costal arch protrusion in sandwich surgery, which was designed for complex thoracic malformations. Although this technique can eliminate the protrusion, it cannot be used for the treatment of independent costal arch deformity. In our clinical practice, we have encountered a large number of patients with single rib arch malformation. In order to treat this special deformity, we designed a minimally invasive procedure. The following is an introduction to this procedure.
Technique
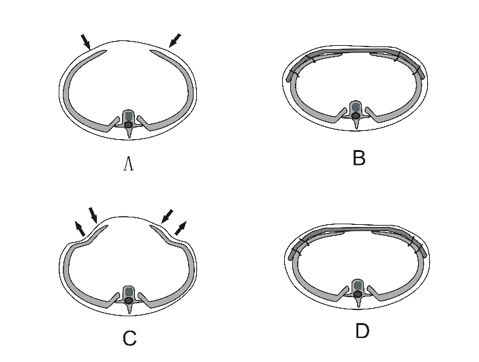
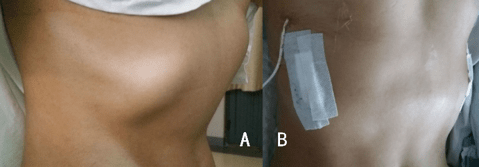
The patient is in supine position, with two upper limbs located in abduction. Two longitudinal skin incisions on both sides of the chest wall are completed, which are equivalent of the costal arch plane. The incisions are located near the axillary midline, about 2cm in length. The subcutaneous tissue and the chest wall muscle are detached, and then one or two tunnels are completed from the incision to the medline of the body, just above the costal arch surface. The tunnel passes through the sheath of the rectus abdominis near the midline and is connected with the tunnel on the other side of the chest wall. For patients with mild anterior protrusion, only one tunnel is enough (Fig 1A, B). For patients with large area protrusion or combined with chest wall depression (Fig 1C), two tunnels are needed, and the distance between tunnels is reasonably arranged according to the scope of deformity. The fixed steel wires are placed surrounding the ribs in tunnel, near the anterior axillary line and axillary midline (Fig 2 A, B). For the deformity combined with depression, the inner steel wire is placed at the lowest part of the depression (Fig 2 C, D). The steel bar is introduced into the tunnel. After the assistant presses down the raised costal arch, the steel bar is fixed in sequence. The wires near the middle line are fixed first, then the wires at both ends of the steel bar are fixed. For the simple protrusion deformities, the bar can be fixed directly. For the deformity with lateral depression, the depression is lifted up by the wire at first, and then fixed to the steel bar. The muscles and subcutaneous tissue are sutured, and the ends of the bar are embedded carefully. After closing the incision, the operation is completed (Fig 3).
Figures
Comment
Deformity at the costal arch is a common malformation of the chest wall, which is often regarded as a part of other thoracic deformities but many of our patients have the solitary costal arch malformation, and they often have strong desire for surgery [2, 3]. There are three forms of independent costal arch deformity: (1) large area protrusion (Fig 1A). The bony structures of the costal arch and the lateral chest wall presents a "slope" shape to the front of the body surface and are higher than the plane of the upper part of the thorax. This is the most common form; (2) local protrusion (Fig 1B). The protruding arch is limited to the costal arch, which area is local, but the deformity is obvious; and (3) combined malformation (Fig 1 C). In addition to the protrusion of costal arch, the lateral chest wall near the costal arch shows a depression, which distorts the local thoracic shape abviously. This is a rare deformity, and it's relatively complicated.
When the costal arch deformity exists with other abnormalities, such as pectus excavatum and puctus carinatum, the deformity can be treated at the same time. The early used method was to remove partial rib arch, and then connect the residual cartilage structures [1]. In 2010, Bosgraaf and colleague introduced a technique for treatment of costal arch deformity after Nuss operation [3]. Different from traditional Ravitch surgery, Nuss surgery is minimally invasive surgery, but the method of Bosgraaf was still the resection of the costal arch structures, and the operation itself is not minimally invasive, so it is not an ideal technique. Lately, Park introduced a "magic string" technique for management of costal arch deformity but was only a part of sandwich surgery designed for complex thoracic deformity [2]. In their technique, a “magic string” was passed through the top of the protrusion at first, and then the two ends of the string were fixed at both ends of the steel bar. After tightening the string, the protrusion was compressed downwards. Such a method is effective in complex malformations, and is a minimally invasive procedure, but it is still an additional procedure. It seems difficult to correct the independent deformity on costal arch. So far, there has been no report on single surgery for independent costal arch deformity.
Our technique, focusing on the independent costal arch deformity, is a minimally invasive surgical method, which is designed to use special steel bar to press the raised costal arch surface. Considering that the deformity is not a simple protrusion, some details have been carefully designed. For the patients with simple protrusion, whether large area or local, satisfactory results can be achieved by using steel bar with suitable shape (Fig 2 A, B). For the combined malformation, which has the depression near the protruding costal arch, the bottom of the depression should be lifted and fixed to the steel bar, so that the satisfactory effect can be achieved (Fig 2 C, D). For rigid, large area deformities, two bars are needed. Our operations are accomplished by two small incisions on the lateral chest wall. Since the incisions are short and their location are hidden, the technique has not only the advantages of minimally invasive surgery, but also an ideal aesthetic effect (Fig 3).
Until now, we have performed this procedure in 9 patients, including 5 cases of large area protrusion, 2 cases of local protrusion, and 2 cases of combined malformation. 6 patients received one bar, and 3 patients received two bars. After the operation, their deformities of costal arch all disappeared, and the appearance returned to normal. No complication occurred. Our experience shows that this method is an ideal minimally invasive surgical technique for the treatment of costal arch deformities.
Article Info
Article Type
Short CommunicationPublication history
Received 25 May, 2018Accepted 7 June, 2018
Published 16 June, 2018
Copyright
© 2018 Wenlin Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.10.31487/j.SCR.2018.02.004
Author Info
Corresponding author
Wenlin WangDepartment of Chest Wall Surgery, Guangdong Second General Provincial Hospital, Guangzhou 510317, P.R.China
Figures & Tables
References
1. Kanagaratnam A, Phan S, Tchantchaleishvilli S, Phan K (2016) Ravitch versus Nuss procedure for pectus excavatum: systematic review and meta-analysis. Ann Cardiothorac Surg 5: 409-421. [Crossref]
2. Park HJ, Kim KS (2016) The sandwich technique for repair of pectus carinatum and excavatum/carinatum complex. Ann Cardiothorac Surg 5: 434-439. [Crossref]
3. Bosgraaf RP, Aronson DC (2010) Treatment of flaring of the costal arch after the minimallyinvasive pectus excavatum repair (Nuss procedure) in children. J Pediatr Surg 45: 1904-1906 [Crossref]