Oral Malodor Knowledge Among Myanmar Dental Students and Young Dentists
A B S T R A C T
Objective: The aim of this study was to evaluate the knowledge of Myanmar dental students and young dentists regarding the diagnosis and treatment of oral malodor.
Method: Data were collected from a sample of 120 dental students from the University of Dental Medicine and 21 young dentists in Yangon, Myanmar. They were instructed to answer the structural questionnaires regarding oral malodor knowledge, including the clinical perspective. The content of the questionnaire items ranged from the etiology of oral malodor to treatment regimen.
Results: Only 8.5% in the dental students’ group and 14.3% in young dentists’ group correctly answered that tongue coating is the most frequent source of oral malodor when the patients had no severe dental and periodontal problems. Nearly half of the subjects reported that Volatile Sulphur Compounds (VSCs) are related to malodor, but only 18.4% correctly answered the question related to the vulnerable condition of VSCs production. And, around 60% of the subjects didn’t know the reliable diagnostic tools for malodor and more than half of the subjects didn’t know clearly about the oral malodor classifications. Regarding the oral malodor treatment, over 90% of the subjects responded tongue cleaning is essential to reduce oral malodor and 97.2% of the subjects answered that they will provide tooth brushing instructions to oral malodor patients. But, over 70% of the subjects incorrectly recommended saline mouthwash for malodor treatment. Overall, both the dental students and young dentists had less knowledge of oral malodor and most of them responded that they need further knowledge on oral malodor diagnosis and treatment.
Conclusion: This study showed that the knowledge of Myanmar dental students and young dentists on oral malodor was a scare. Therefore, it is strongly recommended that dental schools are necessary to give greater emphasis on etiology, diagnosis, and proper treatment for oral malodor.
Keywords
Clinical knowledge, oral malodor, dental students, young dentists, myanmar
Introduction
Oral malodor is an unpleasant smell coming from one’s breath and known as halitosis in the professional term. Nowadays, oral malodor is reported to be the third most frequent reason for people seeking dental care after dental caries and periodontal problems. [1, 2]. Most of the adults had been the victims of oral malodor. It is difficult to evaluate oral malodor prevalence, but previous epidemiological studies on various communities have shown that almost 30%-50% of the population suffers from this problem [3-7]. Oral malodor may cause social embarrassment, stress, and negative influence on daily life [8].
Oral malodor is multifactorial, and it mainly originates from the oral cavity (80%-90%) of all cases [1, 2, 9-11]. Tongue coating, poor oral hygiene, severe periodontal diseases, severe dental caries, and xerostomia are the most frequent association factors for oral malodor production [3, 9, 12-14]. The remaining 10%-20% are caused by systemic diseases, metabolic disorders, food ingestion, and some medications [2, 15, 16]. Therefore, sometimes, oral malodor can be a signal of an individual’s oral hygiene and some systemic health problems. Mostly, oral malodor is caused by a combination of two or more causes. The correct diagnosis is crucial for appropriate management to get patients’ satisfaction with treatment outcomes.
Therefore, thorough asking of the problem history, standard clinical examination, proper diagnosis are essential facts to achieve correct treatment.
Dental professionals are the first line to treat oral malodor, and dentists are frequently asked about oral bad breath by most of the patients. According to a previous study, one-fourth of the dental patients in Myanmar had oral malodor and 40% of dental patients are concerned about their breath odor [3]. Previous studies reported that sometimes dentists don’t know clearly how to evaluate oral malodor problems [17, 18]. It might be because of the lack of the modules related to oral malodor in detail at the undergraduate curriculum. Dental professionals have to know at least a basic knowledge of the etiology, diagnosis, and treatment patterns of oral malodor [16, 19, 20]. Therefore, this study aimed to evaluate the knowledge of etiology, diagnosis and treatment of oral malodor in dental students and young dentists.
Material and methods
This cross-sectional study was conducted in Myanmar dental personnel in Yangon. A structural questionnaire regarding the knowledge of oral malodor was filled by a total sample of 141 final year dental students of the University of Dental Medicine, Yangon and young registered dentists who are working as general dental practitioners in Yangon. This study was designed to access whether dental students and young dentists are being prepared for this issue. The questionnaire related to oral malodor was adopted and modified from Nunes et al. and mainly focuses on the knowledge of etiology, diagnosis, and treatment [18]. Regarding the seven knowledge questionnaires on oral malodor, study participants have to choose one correct answer among given responses. A total score of knowledge was calculated by simply adding the number of correctly answered questions, ranging from 0 to 7. Choice of treatment and effective mouthwash for therapeutic purpose on oral malodor were asked by multiple-answers question type. Statistical analysis was performed using the Statistical Package for Social Science (SPSS version 20). The chi-square test was used to analyze the distributional differences between dental students and dentists. The independent sample t-test was performed to determine the differences in means knowledge scores between groups. A significance level was set at p<0.05. This study protocol was approved by the ethical committee of Tokyo Medical and Dental University (No.850) and authorized by the University of Dental Medicine (Yangon).
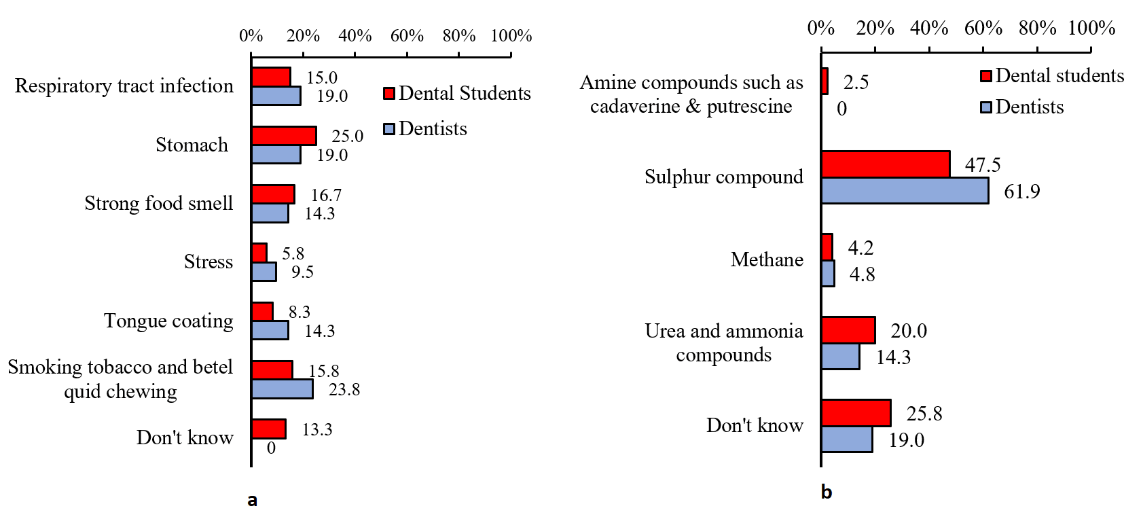

Figure 1: Distribution of the answers to the questions related to oral malodor knowledge. (a) Answers to the question of the most frequent source of oral malodor (without severe periodontal and dental caries problems). (b) Answers to the question of the most frequent volatile compound related to oral malodor. (c) Answers to the question of which oral condition is the most vulnerable to produce oral malodor. (d) Answers to the question of which is considered the most reliable diagnostic tool to detect oral malodor.
Results
The sample was composed of 120 dental students (85.1%) and 21 young dentists (14.9%) and among them, 93 (66%) were male and 48 (34%) were female. The mean age for students and young dentists were 22.0±1.4 and 26.0±4.5 years old, respectively. The proportion of correctly answered on the oral malodor related questionnaires among dental students and dentists were shown in (Table 1). Among the knowledge items, the significant difference (p<0.05) between dental students and dentists was seen only on the question: “Drugs for some systemic diseases are an influence on oral malodor”. Regarding the knowledge questionnaires, the mean of the total knowledge score was 3.43±0.96 in dental students and 4.0±0.78 in dentists, with a statistically significant difference between them (p<0.05). According to the response answers, the percentage of dentists who answered correctly on the questionnaires related to oral malodor is higher than the dental students.
Table 1: Distribution of the correctly responded on the oral malodor knowledge questionnaires.
|
Correctly answered on related oral malodor knowledge |
Proportion of correctly answered |
P - value |
|||
|
Dental Students (N=120) |
Dentists (N=21) |
||||
|
N |
% |
N |
% |
||
|
Tongue coating is the most frequent source of bad breath when the patients had no severe periodontal problems and dental caries. |
10 |
8.3 |
3 |
14.3 |
0.384 |
|
Sulphur compound is the most frequently related volatile compound to oral malodor. |
57 |
47.5 |
13 |
61.9 |
0.223 |
|
Alkaline pH and gram-negative bacteria are the most vulnerable oral conditions to produce oral malodor. |
22 |
18.3 |
4 |
19 |
0.938 |
|
Organoleptic test is the most reliable diagnostic tool and considered as a Gold standard to measure oral malodor. |
5 |
4.2 |
2 |
9.5 |
0.297 |
|
Tongue cleaning is essential to reduce oral malodor. |
112 |
93.3 |
21 |
100 |
0.223 |
|
Oral malodor is influenced by some systemic diseases. |
117 |
97.5 |
21 |
100 |
0.464 |
|
Oral malodor is influenced by some medications for general health problems. |
88 |
73.3 |
20 |
95.2 |
0.029 |
The distribution of the answers on some questions related to oral malodor is stated in (Figure 1). Answer for the question “Which is the most frequent source of oral malodor in patients with no dental and periodontal diseases”, only 8.5% in dental students and 14.3% of dentists can choose tongue coating, correctly. Moreover, only 47.5% in dental students and 61.9% in dentists responded that “sulphur compound” is the most common volatile compound to oral malodor. About 20% of the dental students and dentists knew that alkaline pH and gram-negative bacteria are the most vulnerable oral conditions to produce oral malodor. And also, very few subjects could answer the organoleptic test is the most reliable tool to analyze breath odor.
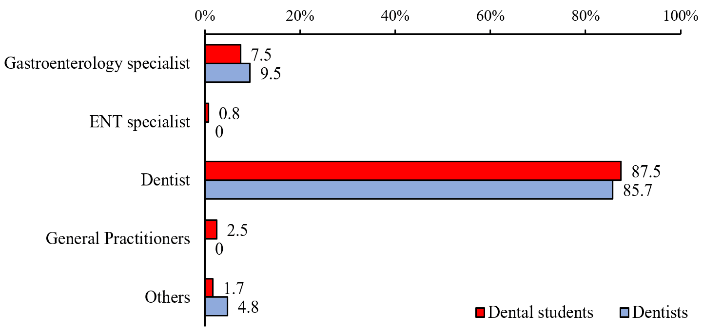
Figure 2: Distribution of the answers on the question of which professional should mainly treat the patients with oral malodor.
In this study, nearly 90% of the participants agreed that the dental personnel is the primary role to treat the patients with oral malodor and the distribution of the answer to this question was shown in (Figure 2). Regarding the treatment, most of the participants chose the oral prophylaxis like scaling and oral hygiene regimes such as toothbrushing, tongue cleaning and mouth washing as an essential treatment for oral malodor, presented in (Figure 3). On the other hand, 74.2% of dental students and 47.6% of dentists mistakenly chose saline mouthwash to recommend for oral malodor, shown in (Figure 4). Nearly all of them, 98.6%, answered that they need to learn further knowledge on oral malodor diagnosis and treatment.

Figure 3: Choice of treatments for patients with oral malodor (multiple answers).
Discussion
Nowadays, people’s concern on oral malodor is increasing and also, oral malodor is one of the main complaints of patients seeking oral healthcare professionals. This is the first study in Myanmar regarding the knowledge of oral malodor on the young dentists and dental students (final year) from the University of Dental Medicine, Yangon. The overall response rate among final year students is nearly 97% except for students who took a leave/ skipped the lecture of the data collection day. As there are only two government Dental Universities (Yangon and Mandalay) in Myanmar and the curriculum are the same within both universities. Therefore, students’ knowledge could represent both universities.

Figure 4: Recommend mouthwashes for oral malodor reduction (multiple answers).
According to the most updated oral malodor related articles and review papers, the oral cavity is the most frequent origin of the oral malodor and gram-negative anaerobes are mainly responsible for oral malodor [2]. A study has been conducted at the bad breath clinic for 7 years period reported that about 4% of the halitosis originated from the extra-oral origin [21]. Volatile Sulphur compounds (VSCs) such as hydrogen sulphide, methyl mercaptan, and dimethyl sulphide is the most associated gas to produce oral malodor, and the organoleptic test is the most reliable to detect oral malodor other than any other tools [1, 2]. Only a few participants in the study can correctly answer the mechanism of oral malodor production, such as the most frequent origin and vulnerable oral conditions. But, half of the sample populations correctly chose that VSCs is the most associated with oral malodor. In this study, the mean scores on knowledge of oral malodor in both dental students and young dentists’ groups were not high. This result was similar to the previous studies had been done in dental professionals’ knowledge on diagnosis and treatment of oral malodor knowledge in Sudan, Portugal, Nigeria and Netherlands [16-19].
Almost 90% of the study population believed that dentists would be the best qualified to be the first to see a patient with bad breath and less than 10% answered that gastroenterology specialists should mainly treat these patients. On the other hand, more than half of the respondents chose the respiratory tract and stomach as the most frequent source of oral malodor rather than oral cavity origin. And also, regarding the treatment, most of the sample populations chose the prophylaxis and oral hygiene regimens including tongue brushing, but the respondents’ knowledge was poor regarding the choice of active compounds in mouthwash for oral malodor reduction. Therefore, the study findings showed that the clinical knowledge of the final year dental students and young dentists regarding the halitosis is insufficient.
According to the previous studies, the prevalence of clinical oral malodor in Myanmar dental patients was 25.5% [3]. So, the clinical knowledge of oral malodor for dental professionals was important to treat the patients’ needs. Low mean knowledge score in young dentists group showed that they also had limited clinical knowledge on oral malodor. Most of the respondents mentioned that they need more knowledge related to oral malodor etiology, diagnosis, and treatment.
There are some limitations to this study. The level of knowledge might be influenced by individual learning performance for dental students and continuous learning performance for young dentists. And also, as the dentists who participated in this study were very limited in numbers and they were young with the average clinical experiences was about 5 years, it should not be represented to overall young dentists’ knowledge level. Except for these limitations, this study findings stated the dental students and young dentists’ level of knowledge on the etiology, diagnosis, and treatment of oral malodor.
Conclusion
As oral malodor is a great deal of important in an individual’s daily life, a lack of confidence by practitioners may lead to dissatisfaction responses from the patients. In this study, dental students and young dentists’ knowledge of oral malodor is inadequate, and they need more knowledge on this issue. Moreover, it is clear that oral health professionals need to be ready to give appropriate and effective treatment to patients who complain about oral bad breath. Therefore, continue education and training to the dental professionals on oral malodor knowledge including the etiology, diagnosis and treatment options are necessary.
Conflicts of Interest
The authors declare that they have no competing interests.
Article Info
Article Type
Research ArticlePublication history
Received: Fri 30, Aug 2019Accepted: Fri 13, Sep 2019
Published: Mon 30, Sep 2019
Copyright
© 2023 Ei Ei Aung. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JDOA.2019.01.02
Figures & Tables
Table 1: Distribution of the correctly responded on the oral malodor knowledge questionnaires.
|
Correctly answered on related oral malodor knowledge |
Proportion of correctly answered |
P - value |
|||
|
Dental Students (N=120) |
Dentists (N=21) |
||||
|
N |
% |
N |
% |
||
|
Tongue coating is the most frequent source of bad breath when the patients had no severe periodontal problems and dental caries. |
10 |
8.3 |
3 |
14.3 |
0.384 |
|
Sulphur compound is the most frequently related volatile compound to oral malodor. |
57 |
47.5 |
13 |
61.9 |
0.223 |
|
Alkaline pH and gram-negative bacteria are the most vulnerable oral conditions to produce oral malodor. |
22 |
18.3 |
4 |
19 |
0.938 |
|
Organoleptic test is the most reliable diagnostic tool and considered as a Gold standard to measure oral malodor. |
5 |
4.2 |
2 |
9.5 |
0.297 |
|
Tongue cleaning is essential to reduce oral malodor. |
112 |
93.3 |
21 |
100 |
0.223 |
|
Oral malodor is influenced by some systemic diseases. |
117 |
97.5 |
21 |
100 |
0.464 |
|
Oral malodor is influenced by some medications for general health problems. |
88 |
73.3 |
20 |
95.2 |
0.029 |
References
- Aydin M, Harvey-Woodworth CN (2014) Halitosis: a new definition and classification. Br Dent J 217: E1. [Crossref]
- Bicak DA (2018) A current approach to halitosis and oral malodor-A mini review. Open Dent J 12: 322-330. [Crossref]
- Aung EE, Zaitsu T, Ueno M (2015) Therapy: Relationship of oral health knowledge, behavior and status with self-perceived and clinical oral malodor among dental patients. J Dent Health Oral Disord Ther 3: 83.
- Liu XN, Shinada K, Chen XC, Zhang BX, Yaegaki K et al. (2006) Oral malodor‐related parameters in the Chinese general population. J Clin Periodontol 33: 31-36. [Crossref]
- Hammad MM, Darwazeh AM, Al-Waeli H, Tarakji B, Alhadithy TT (2014) Prevalence and awareness of halitosis in a sample of Jordanian population. J Int Soc Prev Community Dent 4: S178-S186. [Crossref]
- Rayman S, Almas K (2008) Halitosis among racially diverse populations: an update. Int J Dent Hyg 6: 2-7. [Crossref]
- Rani H, Ueno M, Zaitsu T, Furukawa S, Kawaguchi Y (2015) Factors associated with clinical and perceived oral malodor among dental students. J Med Dent Sci 62: 33-41. [Crossref]
- Sharma S, Shankar T, Koirala B (2011) Halitosis: a serious social problem. Health Renaissance 9: 106-111.
- Morita M, Wang HL (2001) Association between oral malodor and adult periodontitis: a review. J Clin Periodontol 28: 813-819. [Crossref]
- Ratcliff PA, Johnson PW (1999) The relationship between oral malodor, gingivitis, and periodontitis. A review. J Periodontol 70: 485-489. [Crossref]
- Özen M, Aydin M (2015) Subjective halitosis: definition and classification. JNJ Dent Assoc 86: 20-24. [Crossref]
- Aung EE, Ueno M, Zaitsu T, Furukawa S, Kawaguchi Y (2015) Effectiveness of three oral hygiene regimens on oral malodor reduction: a randomized clinical trial. Trials 16: 31. [Crossref]
- Apatzidou AD, Bakirtzoglou E, Vouros I, Karagiannis V, Papa A et al. (2013) Association between oral malodour and periodontal disease-related parameters in the general population. Acta Odontol Scand 71: 189-195. [Crossref]
- De Geest S, Laleman I, Teughels W, Dekeyser C, Quirynen M (2016) Periodontal diseases as a source of halitosis: a review of the evidence and treatment approaches for dentists and dental hygienists. Periodontol 2000 71: 213-227. [Crossref]
- Bollen CML, Beikler T (2012) Halitosis: the multidisciplinary approach. Int J Oral Sci 4: 55-63. [Crossref]
- Adewole RA, Eweka OM, Agbelusi GA (2014) A review of knowledge, diagnosis and treatment of halitosis among Nigerian dentists-a pilot study. Oral Biol Dent 2: 6.
- Khalil I, Hassan K, Kheir EA (2015) Assessment of the Knowledge of Dental Surgeon about Halitosis from Two Dental Teaching Hospitals in Khartoum City. Int Arab J Dent 392: 1-10.
- Nunes JC, Martínez-Sahuquillo Á, Cameira MJ (2011) Halitosis: Are dentists being prepared for this challenge?–A questionnaire survey in a dental school. Revista Portuguesa de Estomatologia, Medicina Dentaria e Cirugia Maxilofacial 52: 142-146.
- Buunk‐Werkhoven YA, Buls JG, Osinga E, Bruers JJ (2015) Diagnosis and treatment of patients with halitosis by dental hygienists and dentists in the Netherlands. Int Dent J 65: 65-70. [Crossref]
- Riaz S, Sultan N, khan ZR (2016) Halitosis: can we treat what we do not understand? Pakistan Oral Dent J 36.
- Zurcher A, Filippi A (2012) Findings, diagnoses and results of a halitosis clinic over a seven-year period. Schweiz Monatsschr Zahnmed 122: 205-216. [Crossref]