Patchwork Flap for Immediate Nipple-Areolar Complex Reconstruction
A B S T R A C T
Loss of nipple projection is commonly encountered during nipple-areolar reconstruction. The patchwork flap was developed to overcome this problem. The thickness of the buried dermofat flap can be modified to the desired nipple projection. Areolar is reconstructed with multiple skin flap islands, which negates the need for skin grafting. The dimensions of the skin islands can be modified to the desired areolar size.
Keywords
Nipple reconstruction, nipple-areolar reconstruction, nipple projection, breast reconstruction
Introduction
The patchwork flap provides control over nipple projection and areolar dimensions. Nipple reconstruction is based on the C-H flap [1]. Areolar is reconstructed with multiple islanded skin flaps. We report a case of immediate nipple reconstruction using the patchwork flap during transverse rectus abdominis myocutaneous flap reconstruction of a mastectomy defect.
Technique
The vertical dimension of the flap corresponds to the contralateral NAC plus the width of the H-flap. The horizontal dimension of the flap corresponds to the horizontal dimension of the contralateral NAC plus 5mm to account for the dermofat flap. The horizontal and vertical length of the areolar can be adjusted by trimming the edges of the skin islands. Areolar prominence at the nipple base can be increased by de-epithelializing the edges of the skin islands and burying them during the closure. The C-H flap is elevated as described previously [1]. The area of dermofat flap is de-epithelialized and elevated until the C flap is reached. It is trimmed based on the desired nipple projection. It is rolled and buried within the C-H flaps. The closure is achieved with interrupted buried dermal stitches and fast-absorbing skin stitches (Figure 1).
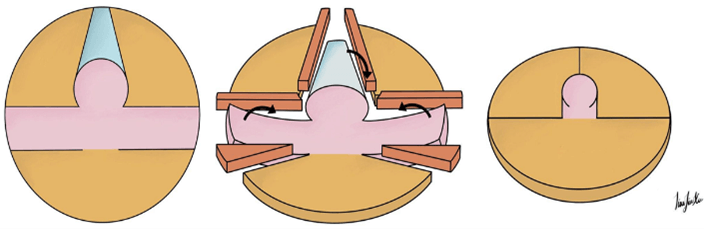
Figure 1: (Left) Incision markings: Pink denotes C-H flap for nipple reconstruction; Brown denotes skin islands for areolar reconstruction; Blue denotes vascularized dermofat flap for nipple projection. (Middle) Skin islands and flaps elevated. Areas shaded in orange represent parts of the skin islands that can either be: i) De-epithelialized and buried within the C-H flap base for increased nipple base projection; ii) Excised and discarded to modify the dimensions of the areola. Dermofat flap is rolled and buried within the C-H flap. (Right) Reconstructed nipple-areolar complex.
Discussion
The patchwork flap reconstructs the areola without skin grafting. This is a modification of a previously described technique of a double opposing nipple-areolar flap [2]. Vascularized dermofat flap provides greater control over nipple projection. Areolar prominence is increased by burying de-epithelialized edges of the skin islands. Areolar dimensions are controlled by varying the size of areolar skin islands. These improve structural support, reducing loss of projection which is a common problem faced during nipple-areolar complex reconstruction [3]. Early experience shows no loss of projection and good retention of size at up to two years follow-up (Figure 2).

Figure 2: Reconstructed nipple-areolar complex with the patchwork flap shows retention of nipple projection at 1cm, even after radiation therapy. This patient underwent skin-sparing mastectomy of the right breast, with immediate pedicled transverse rectus abdominis myocutaneous (TRAM) flap reconstruction.
Conclusion
Nipple projection and areolar dimensions can be easily controlled using the patchwork flap.
Acknowledgment
We would like to thank Dr Jia Xu Lim, from the Department of Neurosurgery, National Neuroscience Institute, Singapore, for his contribution to the article’s artwork.
Conflicts of Interest
None.
Article Info
Article Type
Short ReportPublication history
Received: Wed 06, Jan 2021Accepted: Thu 21, Jan 2021
Published: Mon 01, Feb 2021
Copyright
© 2023 Elijah Z. Cai. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2021.02.01
Figures & Tables
References
- Thomas SV, Gellis MB, Pool R (1996) Nipple reconstruction with a new local tissue flap. Plast Reconstr Surg 97: 1053-1056. [Crossref]
- Shestak KC, Nguyen TD (2007) The double opposing periareola flap: a novel concept for nipple-areola reconstruction. Plast Reconstr Surg 119: 473-480. [Crossref]
- Gougoutas AJ, Said HK, Um G, Chapin A, Mathes DW (2018) Nipple-Areola Complex Reconstruction. Plast Reconstr Surg 141: 404e-416e. [Crossref]