Pediatric Cecal Volvulus: A Case Report
A B S T R A C T
Introduction: Cecal volvulus (CV) is rare cause of intestinal obstruction especially in children. There is no established protocol for the treatment of CV due to its rarity.
Case Presentation: We present a rare case of CV in a 9-year-old girl.
Discussion: The spectrum of intestinal malrotation may give rise to a mobile cecum that may result to CV. Constipation could be a predisposing factor. The clinical presentation which may include abdominal pain, distension, constipation and vomiting depends on the time of presentation. There may be associations with chromosomal abnormalities.
Conclusion: Although CV is a rare cause of intestinal obstruction, awareness and high index of suspicion is needed by clinician for early diagnosis and treatment.
Keywords
Cecal volvulus, pediatric, case report
Introduction
Cecal volvulus (CV) is a rare cause of intestinal obstruction in children and the exact incidence is unknown [1]. CV results from abnormal intestinal rotation and fixation that occurs during intrauterine life, which leads to cecal mobility [2]. On a background of a mobile cecum, psychomotor retardation and chronic constipation may be predisposing factors [3]. The clinical presentation of CV is variable and depends on the pattern, severity and duration of the volvulus. These non-specific presentations make preoperative diagnosis difficult [4]. The options of treatment of CV range from cecopexy to intestinal resection. Delayed treatment of CV may result in strangulation, ischaemia and gangrene [5]. We present a case of cecal volvulus in a 9-year-old female who had no intra-peritoneal evidence of intestinal malrotation.
Case Presentation
A 9-year-old girl presented with 3 days history of abdominal pain, 2 days of constipation and a day of bilious vomiting. There was no history of chronic constipation preceding the above symptoms and she has normal developmental milestone appropriate for her age. The patient has not had a similar episode of the above symptoms in the past. On examination, she was well nourished and in moderate painful distress. The abdominal pain waxes and wanes (colicky) and was relieved by taking analgesics. The vitals were pulse rate 82 beats per minute, full volume, regular; blood pressure 85/60 mmHg; respiratory rate 23 cycles per minutes; Temperature 37°C; SP02 98% at room air. Abdomen was full, moves with respiration with visible bowel loops. Although there was no guarding and no rigidity, the periumbilical region was mildly tender. The liver and spleen were not palpable; kidneys were not ballotable. Bowel sounds were hyperactive. The rectum was empty on digital rectal examination. Other systems were essentially normal.
Laboratory investigations showed a full blood count of within normal range. Serum electrolytes, urea and creatinine were not deranged. Urinalysis, retroviral and hepatitis B screening showed no abnormality. Plain abdominal x-ray showed air fluid levels with most of the abdomen gasless (Figure 1). Contrast studies of the intestinal tract and abdominal computed tomography scan were not done because the patient could not afford them. Based on the above findings, a working diagnosis of intestinal obstruction of unknown cause was made. The patient was resuscitated, optimized and informed consent obtained from the caregivers. The intra-operative finding at laparotomy was 180-degree counter-clockwise volvulus of the cecum which showed patchy areas of pigmentation (Figure 2). The duodenojejunal junction and cecum were normally located in the left side of the midline and right lower quadrant respectively (no malrotation). On account of the appearance of the cecum, a right hemicolectomy with ileotransverse anastomosis was performed. The post-operative period was uneventful, and the patient was discharged home on the 10th post-operative day. She has been followed up for 6 months and has not shown any post-operative complications.

Figure 1: Plain abdominal x-ray showing multiple air fluid levels.
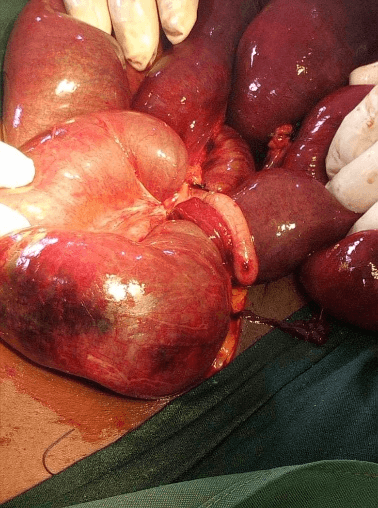
Figure 2: Intra-operative picture showing the cecal volvulus with pigmented areas.
Discussion
CV is an uncommon cause of intestinal obstruction. In adults, CV account for about 1% of all cases of intestinal obstruction and 30% of cases of large bowel volvulus [6, 7]. The exact incidence of CV in children is unknown due to extremely rare occurrence of CV in children. Intestinal malrotation, which is a spectrum of intestinal rotation and fixation, is the cardinal event that creates a mobile cecum which predisposes it to volvulus. The diagnosis of CV can be challenging because the pattern of presentation varies from one patient to another and preoperative diagnosis is rarely achieved in most cases [4]. CV can also occur as a post-operative complication of certain surgeries like nephrectomy for Wilms’ tumor [8]. However, this is an unusual complication because post-operative adhesions and intussusception have been reported as the most common causes of intestinal obstruction following nephrectomy [9]. Children who have developmental delays and chromosomal disorders such as trisomy 17 are also at risk of having CV [10].
In terms of investigations, abdominal radiograph is the initial diagnostic test and is usually abnormal. In the index case, there were multiple air fluid levels which support intestinal obstruction but there was nothing specific about CV. However, one study reported that 50% of the cases of CV can be detected through abdominal radiographs [4]. Abdominal ultrasound may be useful in evaluating for differential diagnosis of CV, but ultrasound is not reliable enough to exclude the diagnosis. Ultrasound was not helpful in the index case. Computed tomograghy scan, which give more details, is currently used for more accurate diagnosis and to differentiate CV from other acute emergent conditions. Howbeit, computed tomography scan should be used with caution in children due to the risk of exposure to radiations [4]. Our patient did not get computed tomography scan due to its non-availability and non-affordability. Laparotomy or laparoscopy is the only absolute modality of making absolute diagnosis [11].
There are options of management of CV. These include cecopexy, simple detorsion without fixation, detorsion with cecopexy, tube cecostomy and surgical resection in the form of right hemicolectomy [12]. We offered our patient right hemicolectomy due to pigmented patches on the cecum. The treatment of CV should be individualized and may depend on the state of the cecum, experience of the surgeon and available facilities. For patients with comorbidity who may not withstand surgery under general anaesthesia, there is a place for colonic decompression [3]. However, the authors advised that colonoscopy should only be performed in stable patients without bowel compromise or perforation [3].
Conclusion
CV is a very rare cause of intestinal obstruction in children. Clinicians should be aware of this entity because delayed presentation or late treatment may lead to bowel gangrene and fatal complications.
Article Info
Article Type
Case ReportPublication history
Received: Mon 01, Jun 2020Accepted: Wed 17, Jun 2020
Published: Tue 30, Jun 2020
Copyright
© 2023 Chukwubuike Emeka. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.AJSCR.2020.02.13
Figures & Tables
References
- Miura da Costa K, Saxena AK (2018) A systematic review of the management and outcomes of cecal and appendiceal volvulus in children. Acta Paediatr 107: 2054-2058. [Crossref]
- Robert JT, Edwin IS (1998) Pediatric Surgery. In: James AN Jr, Marc IR, Jay LG, Eric WC, Arnold CG, editors. Pediatric Surgery. 5th ed. Missouri: Mosby Publications 1203-1207.
- van de Lagemaat M, Blink M, Bakx R, de Meij TG (2018) Cecal Volvulus in Children: Is There a Place for Colonoscopic Decompression? J Pediatr Gastroenterol Nutri 66: e59-e60. [Crossref]
- Hasbahceci M, Basak F, Alimoglu O (2012) Cecal volvulus. Indian J Surg 74: 476-479. [Crossref]
- Takada K, Hamada Y, Sato M, Fujii Y, Teraguchi M et al. (2007) Cecal volvulus in children with mental disability. Pediatr Surg Int 23: 1011-1014. [Crossref]
- Ballantyne GH, Brandner MD, Beart RW Jr, Ilstrup DM (1985) Volvulus of the colon. Incidence and mortality. Ann Surg 202: 83-92. [Crossref]
- Habre J, Sautot Vial N, Marcotte C, Benchimol D (2008) Caecal volvulus. Am J Surg 196: e48-e49. [Crossref]
- Gonzalez Urquijo M, Ovalle Chao C, Flores Villalba E, de Jesus Garza Luna U, Velazco De La Garza JH et al. (2018) Cecal Volvulus following a Right Nephrectomy for Wilms’ Tumor: Should We Need to Close the Lateral Peritoneum? European J Pediatr Surg Rep 6: e1-e3. [Crossref]
- Ritchey ML, Kelalis PP, Etzioni R, Breslow N, Shochat S et al. (1993) Small bowel obstruction after nephrectomy for Wilms’ tumor. A report of the National Wilms’ Tumour Study -3. Ann Surg 218: 654-659.
- Phillips G, Parisi MT (2010) Cecal volvulus: classic imaging appearance of an uncommon pediatric entity. Pediatr Radiol 40: S98. [Crossref]
- Millar AJ, Rode H, Cywes S (2003) Malrotation and volvulus in infancy and childhood. Semin Pediatr Surg 12: 229-236. [Crossref]
- Rabinovici R, Simansky DA, Kaplan O, Mavor E, Manny J (1990) Cecal volvulus. Dis Colon Rectum 33: 765-769. [Crossref]