Primary Clear Cell Sarcoma of Bone: Report of a Case Arising from Distal Femur in a Pediatric Patient and Review of the Literature
Primary Clear Cell Sarcoma of Bone: Report of a Case Arising from Distal Femur in a Pediatric Patient and Review of the Literature
A B S T R A C T
Clear cell sarcoma is a rare mesenchymal tumor with melanocytic differentiation, firstly described by Enziger in 1965. It accounts for less than 1% of all soft tissue sarcomas and occurs predominantly in the extremities of adults. Primary clear cell sarcoma of bone is even rarer; current literature consists of only 13 cases with a mean age of presentation of 45-year-old, ranging from 18 to 81. Because of the overlapping expression of melanocytic markers, the differential diagnosis should be addressed with metastatic malignant melanoma and metastasis from clear cell sarcoma of soft parts. Essential for the diagnosis is the evidence of translocations t (12;22) or t (2;22) resulting respectively in EWSR1/ATF1 and EWSR1-CREB1 gene fusion. Clinical history and radiological assessment could help discriminate between bone or soft parts origin. We report an unusual case of clear cell sarcoma of distal femur involving a 13-year-old patient. Histological sections showed a malignant neoplasm composed of nests of uniform cells separated by fibrous septa, showing strong immunoreactivity for melanoma triple cocktail. Real Time-Polymerase Chain Reaction revealed the presence of the fusion product EWSR1-ATF1, confirming the diagnosis of clear cell sarcoma of bone. Our purpose was to revise the current literature in order to find common clinical-radiological features to this rare entity. To the best of our knowledge, our case is the first bone clear cell sarcoma arising from the distal femur in a pediatric patient described in the literature: it highlights the importance of considering this rare entity in the differential diagnosis of primary bone tumor, although extremely rare and of the use of molecular means to confirm the diagnosis.
Keywords
Bone clear cell sarcoma, primary bone tumor, t (12;22) translocation, EWSR1/ATF1 genes fusion
Introduction
Clear cell sarcoma (CCS) is a rare mesenchymal tumor accounting for less than 1% of all sarcomas, mainly arising from deep soft tissues near tendons and aponeurosis of the extremities, above all foot and ankle, with a peak of incidence in young adults, between 20-40 years of age. Enziger described it first in 1965 [1]. Due to its characteristic expression of melanocytic markers (HMB-45, S-100, MelanA), overlapping with malignant melanoma (MM) immunological profile, it was previously known as MM of soft parts. Nevertheless, the presence of chromosomal translocations t (12;22) in about 90% of CCS and less frequently t (2;22), resulting respectively in EWSR1-ATF1 and EWSR1-CREB1 genes fusions, confirms the diagnosis of CCS, since these translocations are absent in MM and other mimickers [2-5].
Primary CCS of bone is its rarer form originating from the bone, which shares the same morphological, immunohistochemical, and molecular features. Due to its extreme rarity, imaging appearance, and histological pattern similar to other entities (like soft tissue CCS and MM), differential diagnosis is challenging and must include mainly a metastatic MM and a bone metastasis or secondary bone involvement from soft tissue CCS. The mainstay in the differential diagnosis of CCS of the bone with other bone entities and MM is based on the positivity of rearrangement EWSR1-ATF1, whereas with soft tissues CCS only on clinical and radiological features. From a radiological point of view, the majority of cases reported shared a pure lytic bone lesion with cortical disruption and secondary soft tissue involvement. Bone scan and 18F-labeled fluoro-2-deoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) are essential to pathological staging and detection of distant locations when ruling out metastatic MM or soft tissue CCS. To date, only 13 cases described as primary CCS of bone have been reported in literature: in 1996, first described a case in the ulna; other presented cases were from ribs, sternum, metatarsal bone, radius, scapula, humerus, sacrum, pubis and calcaneus [6-18]. No cases have been reported before in long bones of the lower limb or in pediatric age and upon critical review, only 3 of 13 were shown to harbour t (12;22) translocation, while the remaining cases were not confirmed by molecular analysis. Furthermore, in our opinion, one case reported as CCS arising from third metatarsus did not really originate from bone, as shown by the diagnostic imaging reported by authors (Table 1) [12].
Table 1: Overview and comparison between previously reported cases of clear cell sarcoma of bone in literature.
|
Authors |
Age |
Sex |
Location |
Radiographic pattern |
Translocation |
Treatment |
Relapse |
Follow-up (mo) |
Status |
|
Yokoyama et al. (1996) |
33 |
F |
Epiphyseal |
Lytic |
Not available |
NeoAd CT+RT, Surgery, AdCT |
None |
65 |
NED |
|
Gelczer et al. (1999) |
18 |
M |
Diaphyseal |
Lytic |
Not available |
Surgery, AdCT
|
LocRec
|
55 |
NED |
|
Hersekli et al. (2005) |
28 |
F |
Diaphyseal |
Lytic |
Negative |
Surgery, AdCT
|
None |
33 |
NED |
|
Rocco et al. (2009) |
53 |
M |
Sternum |
Lytic |
Positive |
Surgery |
None |
3 |
NED |
|
Brekke et al. (1998) |
62 |
F |
Meta-Epiphyseal |
Lytic |
Not available |
Surgery (amputation) |
None |
15 |
NED |
|
Choi et al. (2003) |
48 |
F |
Epiphyseal |
Lytic |
Not available |
Surgery (amputation) |
Bone Met |
20 |
DOD |
|
Licata et al. (2014) |
42 |
M |
Metaphyseal |
None |
Not available |
Surgery (amputation) |
- |
- |
- |
|
Inaoka et al. (2013) |
55 |
M |
Meta-Epiphyseal Radius |
Lytic |
Negative |
NeoAdCT, Surgery |
LN Mets* |
18 |
NED |
|
Kazakos et al. (2006) |
61 |
M |
Scapula |
Lytic |
Not available |
Surgery, AdCT |
Lung Mets |
10 |
DOD |
|
Liu et al. (2011) |
20 |
F |
Metaphyseal |
Lytic |
Negative |
Surgery, AdCT |
None |
24 |
NED |
|
Zhang et al. (2011) |
25 |
M |
Sacrum |
Lytic |
Positive |
Surgery (curettage) |
LocRec |
9 |
AWD |
|
Nakayama et al. (2012) |
81 |
M |
Pubis |
Lytic |
Negative |
Palliative CT |
- |
- |
DOD |
|
Xu et al. (2019) |
61 |
M |
Calcaneus |
Lytic |
Positive |
Surgery (amputation) |
Lung Mets |
6 |
AWD |
|
Lana et al. (2020) |
13 |
M |
Meta-Epiphyseal |
Lytic |
Positive |
NeoAdCT+ Surgery+ AdCT |
Lung+BoneMets |
8 |
AWD |
NeoAd CT: Neoadjuvant Chemotherapy; AdCt: Adjuvant Chemotherapy; RT: Radiation Therapy; Mets: Metastasis; LN: Lymph Nodes; LocRec: Local Recurrence; NED: No Evidence Of Disease; AWD: Alive With Disease; DOD: Dead Of Disease; * excision at 6 months; - : not specified.
Case Report
We report the case of a 13-year-old Caucasian patient with 2 months history of right knee pain not associated with previous trauma, who was referred to our institution from another hospital. The patient and his family were informed that data from the case would be submitted for publication and gave their consent. Clinically he presented a hard swelling at the medial condyle of the right femur. The range of motion was normal and there were no vascular or neurological deficits. Radiographs and computed tomography (CT) of the right knee put in evidence an ill-defined osteolytic lesion of the medial femoral condyle which spreads over the growth plate with a geographic pattern cortical disruption and limited extra-compartmental involvement (Figures 1-3). A CT guided core needle biopsy was performed and the 18F-FDG PET/CT for pathology staging confirmed the lytic lesion (42x29 mm) with focal and unique increased metabolic activity (SUV= 5.96) (Figures 4 & 5). Lung CT scan resulted negative for metastases. The histopathological diagnosis performed elsewhere was “Ewing sarcoma,” and consequently the patient started neoadjuvant chemotherapy with Vincristine 1,5mg/mp in pump infusion for 24 hours + Ifosfamide 3g/mp/day and Etoposide 150mg/mp/day for 72 hours (VIDE protocol). The Second session of chemotherapy was administrated with the same drugs at lower doses of 25%. Third session of chemotherapy included Vincristine 2mg/mp/day in pump infusion for 24 hours, Cyclophosphamide 600mg/mp/day for 48 hours and Doxorubicin 37,5 mg/mp/day for 48 hours (VDC protocol). He was then referred to our institution for surgical treatment.

Figure 1: a) Preoperative antero-posterior and b) lateral view radiographs: lytic bone lesion with geographic cortical destruction pattern at the medial condyle of the right femur spreading through the growth plate, without evidence of periosteal reaction.
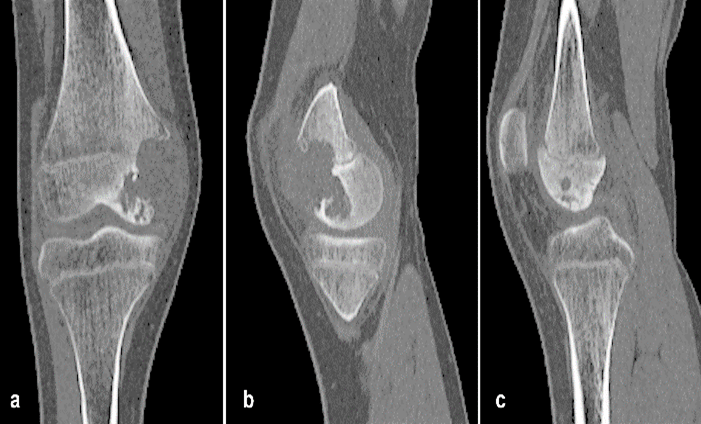
Figure 2: a) Preoperative coronal and b) sagittal computed tomography. Presence of osteolytic lesion at medial femoral condyle spreading over the growth plate, with a geographic pattern of disruption and a homogeneous signal intensity. No evidence of periosteal reaction.
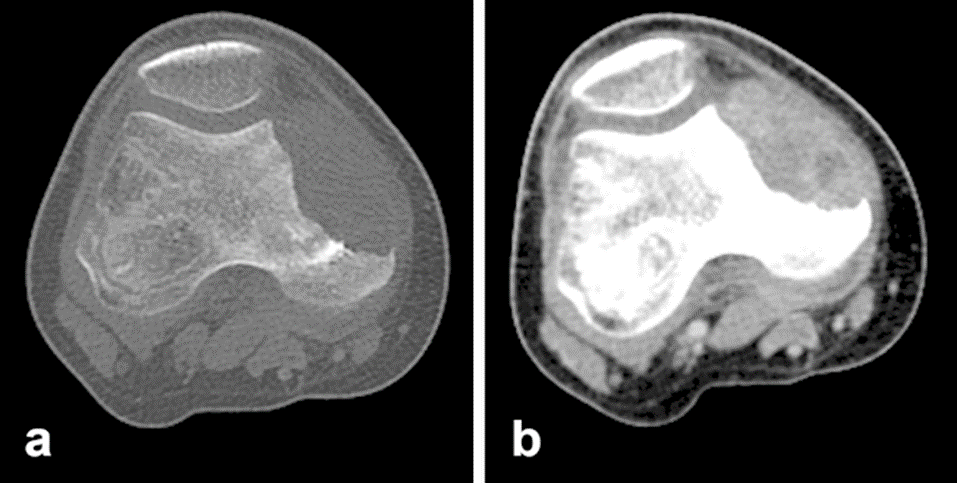
Figure 3: a) Preoperative axial computed tomography without and b) with injection of medium contrast. The image on the left is possible to appreciate the diffuse and homogeneous uptake of medium contrast.
The first core needle biopsy sections were revised by our pathologists. The histological sections showed a malignant neoplasm composed by nests of uniform cells separated by fibrous septa. The neoplastic cells were polygonal, small to medium-sized, exhibited amphophilic or clear cytoplasm and atypical vesicular nuclei with macronucleoli. The tumor cells showed diffuse and strong immunoreactivity for melanoma triple cocktail (HMB-45+A103+T311), anti-MART1 and MITF; they were focal and weakly positive for anti-HMB-45 and negative for CD99, CK AE1/AE3, Desmin, Myogenin, CCNB3 and BCOR (Figures 6a, 6b & 6c). At the light of the melanocytic immunophenotype of the neoplasm, Real Time-Polymerase Chain Reaction (RT-PCR) for the research of the fusion product EWSR1-ATF1 resulting from the reciprocal translocation t (12;22) (q13;q12) was performed and resulted positive, confirming a diagnosis of CCS (Figure 6e). Taking into account the histological, immunohistochemical and molecular pattern of the neoplasm, its location and radiological aspect, we concluded that the neoplasm should be regarded as a rare case of primary CCS of bone. The young patient underwent wide resection of the distal right femur and reconstruction with a modular prosthesis (Figures 7a & 7b).
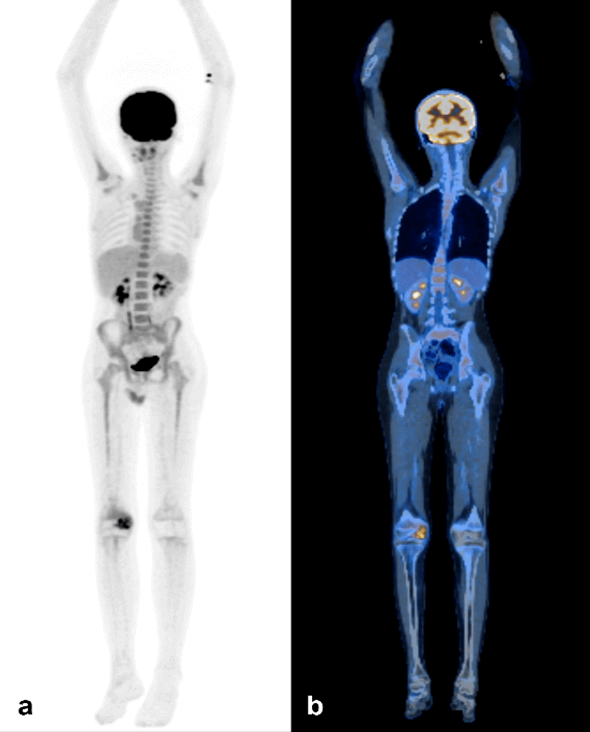
Figure 4: a) 18F-FDG PET and b) overlapping images 18F-FDG PET/CT: no evidence of other pathological accumulation rather than right distal femur (SUV max 5.96).
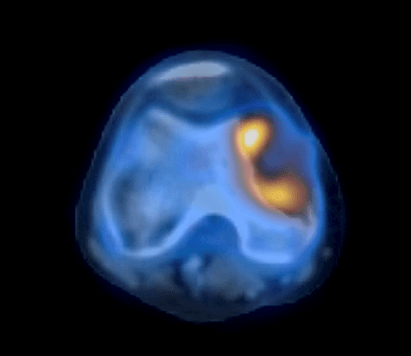
Figure 5: Particular of 18F-FDG PET/CT on the right distal femur.
The surgical specimen of distal femur resection showed areas similar to those found in the biopsy, but also others of spindling with monomorphic neoplastic cells exhibiting clear cytoplasm and arranged in a nested pattern (Figures 6a & 6b). There was limited necrosis (<10%) and the mitotic count was low. Interspersed wreath-like giant cells were conspicuous. Extensive permeation of malignant cells through trabecular bone and cortical breaching with peri-osseous soft tissue infiltration was evident (Figure 6d). The patient did not undergo adjuvant chemotherapy in light of the definitive diagnosis and the poor histological response to the neoadjuvant one. At 3 months from surgery, there was no evidence of disease. At last clinical-radiological follow-up, 8 months from surgery, the CT scan put in evidence multiple lung and bone metastasis, the latter located in thoracic and upper lumbar vertebral bodies: consequently, the patient has been addressed to adjuvant chemotherapy.
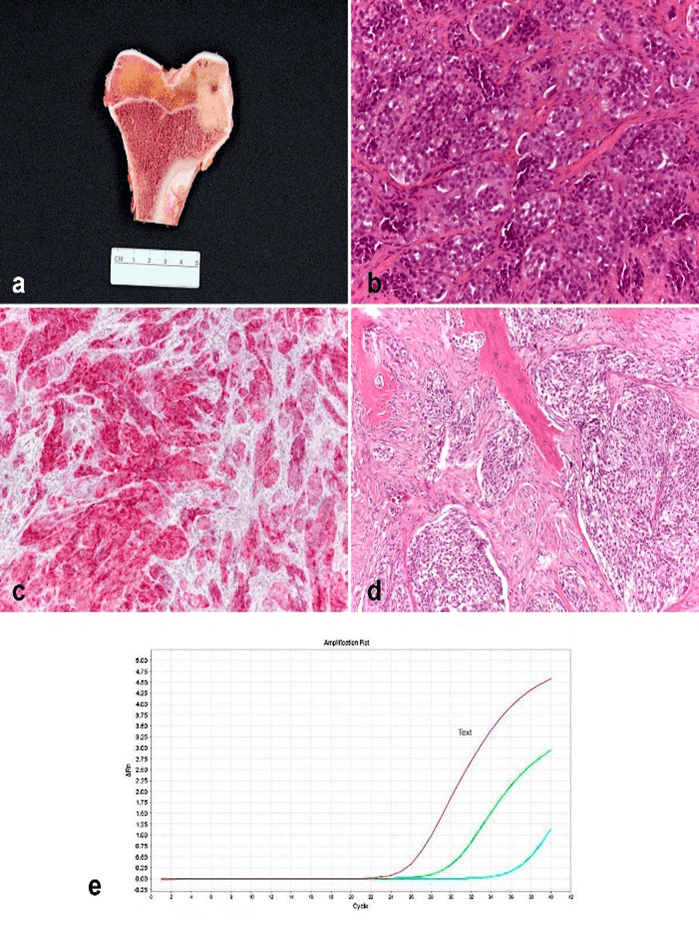
Figure 6: Gross, microscopic, immunohistochemical and molecular features of the tumor: a) resection specimen of right distal femur exhibiting an eccentric meta-epiphyseal lesion measuring 3.0 cm in largest dimension. b) Histologic section of biopsy specimen showing nests of uniform cells separated by fibrous septa (H&E, ×200 magnification). c) Melanin cocktail strong and diffuse immunoreactivity (×100 magnification). d) Representative area of the resection specimen showing permeation of trabecular bone by nests of spindle tumor cells with clear cytoplasm (×100 magnification). e) RT-qPCR amplification plot shows the positive results for EWSR1-ATF1 gene fusion (green line) compared to the housekeeping gene (red line).
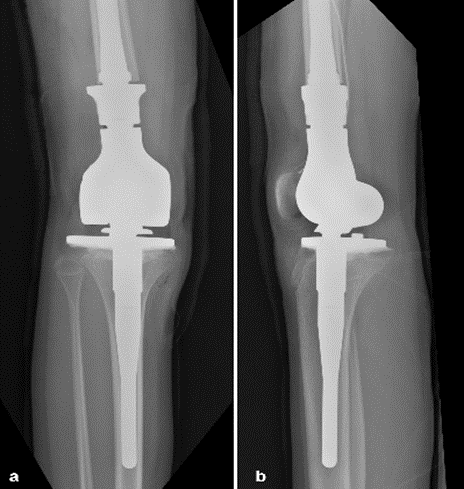
Figure 7: a) Post-operative antero-posterior and b) lateral view radiographs.
Discussion
Primary CCS of bone is an extremely rare primary tumor of uncertain histological origin. The literature on bone CCS consists to date of only 13 single case reports with a mean age of presentation of 45-year-old, ranging from 18 to 81. The sites of presentation vary from axial to appendicular skeleton, but in the cases, which involved long bones, the tumor seemed to occur most frequently in the meta-epiphyseal region. Only 3 cases have molecular confirmation with positivity to translocation t (12;22) (q13; q12); on the contrary, 4 patients were negative and in 6 cases this information lacked, undermining the veracity of the diagnosis. Furthermore, from our critical review one case seemed to originate from soft tissues rather than from bone [12] (Table 1).
As for soft tissue CCS, histologically exhibits round or spindle neoplastic cells with clear to moderate eosinophilic cytoplasm, organized in nests or short fascicles separated by dense collagenous septa. Their nuclei are round and uniform, often with large nucleoli [4]. Scattered wreath-like multinucleated giant cells are generally present. Neoplastic cells show immunohistochemical positivity for melanocyte-specific markers (HMB-45 and Melan-A), MITF, tyrosinase and S-100 protein. Typically, Cyto-Keratin AE1-3, EMA, Smooth muscle actin (SMA) and Desmin are negative, although cases with aberrant immunophenotype have been reported [19].
Genetically, is characterized by the presence of t (12; 22) (q13; q12) translocation, that leads to the fusion of activating transcription factor1 (ATF1) oncogene on chromosome 12q13 and Ewing sarcoma oncogene (EWSR1) on chromosome 22q12, resulting in the EWSR1-ATF1 fusion protein [4, 5]. It is not known, due to the poor number of cases described in the literature, if translocation t (2;22) (q34; q12), resulting in EWSR1-CREB1 gene fusion, reported in a minority of soft tissue CCS, is expressed in CCS of bone as well [4, 18, 19]. From a radiological point of view, all the cases reported of CCS of bone shared the same radiological aspects of pure lytic bone lesion, sometimes breaking through the cortex in a geographic pattern and infiltrating the surrounding soft tissues, like in the case we describe.
According to our retrospective analysis of the cases reported so far and including ours, the most frequent treatment was wide surgical resection, as the mainstay of treatment for the vast majority of primary bone sarcomas, except for the cases of foot bone involvement in which amputation was performed. Clinical course is unfavorable with progression in almost 50% of the cases, with lung being the most frequent site of metastases. Contrary to soft tissue CCS, nodal involvement is not frequent (7,1% vs. 29%) (Table 1) [4]. Overall, since no effective chemotherapy is feasible, prognosis of patients affected by CCS of bone is still poor and, with the limit of a retrospective analysis, 42,8 of the patients died at follow-up or were alive with disease at a mean follow-up time of respectively 15 and 7,6 months (Table 1).
Currently, with the lack of a wider clinical experience on a larger cohort of patients, surgery appears to be the only beneficial treatment, with the hope that new therapeutic agents and targeted molecular therapy will be implemented to improve the oncologic outcome in both early and late stages disease. To the best of our knowledge, the present case is the first CCS of bone described in the pediatric age and the first one arising from femur. Although extremely rare, CCS of bone should be considered in the differential diagnosis of primary bone tumors.
Declarations
Written informed consent was obtained from the subject and his parents before publishing the study. We the authors of this submission confirm that we have not published the same or a very similar study with the same or very similar results and major conclusions in any other journals. These include English or non-English language journals and journals that are indexed or not indexed in PubMed, regardless of different words being used in the article titles, introduction, and discussion.
Author Contributions
All authors declare that:
i. All Authors contributed to conception and design, acquisition of data, analysis, and interpretation of data.
ii. All Authors participated in drafting the article or revising it critically for important intellectual content.
iii. All Authors gave final approval of the version to be submitted and any revised version.
Concerning the specific contributions,
i. Debora Lana: Conceiving the original idea, investigation and revision of literature, manuscript writing.
ii. Marina Pacheco and Marco Gambarotti: Histologic section and interpretation of results.
iii. Federico Ostetto: Help in data collection.
iv. Stefania Benini: Molecular analysis.
v. Davide Maria Donati: Revision of the manuscript.
vi. Giuseppe Bianchi: Revision of the manuscript.
Conflicts of Interest
None.
Funding
None.
Article Info
Article Type
Case Report and Review of the LiteraturePublication history
Received: Thu 20, Aug 2020Accepted: Thu 03, Sep 2020
Published: Wed 30, Sep 2020
Copyright
© 2023 Debora Lana . This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.09.10
Figures & Tables
Table 1: Overview and comparison between previously reported cases of clear cell sarcoma of bone in literature.
|
Authors |
Age |
Sex |
Location |
Radiographic pattern |
Translocation |
Treatment |
Relapse |
Follow-up (mo) |
Status |
|
Yokoyama et al. (1996) |
33 |
F |
Epiphyseal |
Lytic |
Not available |
NeoAd CT+RT, Surgery, AdCT |
None |
65 |
NED |
|
Gelczer et al. (1999) |
18 |
M |
Diaphyseal |
Lytic |
Not available |
Surgery, AdCT
|
LocRec
|
55 |
NED |
|
Hersekli et al. (2005) |
28 |
F |
Diaphyseal |
Lytic |
Negative |
Surgery, AdCT
|
None |
33 |
NED |
|
Rocco et al. (2009) |
53 |
M |
Sternum |
Lytic |
Positive |
Surgery |
None |
3 |
NED |
|
Brekke et al. (1998) |
62 |
F |
Meta-Epiphyseal |
Lytic |
Not available |
Surgery (amputation) |
None |
15 |
NED |
|
Choi et al. (2003) |
48 |
F |
Epiphyseal |
Lytic |
Not available |
Surgery (amputation) |
Bone Met |
20 |
DOD |
|
Licata et al. (2014) |
42 |
M |
Metaphyseal |
None |
Not available |
Surgery (amputation) |
- |
- |
- |
|
Inaoka et al. (2013) |
55 |
M |
Meta-Epiphyseal Radius |
Lytic |
Negative |
NeoAdCT, Surgery |
LN Mets* |
18 |
NED |
|
Kazakos et al. (2006) |
61 |
M |
Scapula |
Lytic |
Not available |
Surgery, AdCT |
Lung Mets |
10 |
DOD |
|
Liu et al. (2011) |
20 |
F |
Metaphyseal |
Lytic |
Negative |
Surgery, AdCT |
None |
24 |
NED |
|
Zhang et al. (2011) |
25 |
M |
Sacrum |
Lytic |
Positive |
Surgery (curettage) |
LocRec |
9 |
AWD |
|
Nakayama et al. (2012) |
81 |
M |
Pubis |
Lytic |
Negative |
Palliative CT |
- |
- |
DOD |
|
Xu et al. (2019) |
61 |
M |
Calcaneus |
Lytic |
Positive |
Surgery (amputation) |
Lung Mets |
6 |
AWD |
|
Lana et al. (2020) |
13 |
M |
Meta-Epiphyseal |
Lytic |
Positive |
NeoAdCT+ Surgery+ AdCT |
Lung+BoneMets |
8 |
AWD |
NeoAd CT: Neoadjuvant Chemotherapy; AdCt: Adjuvant Chemotherapy; RT: Radiation Therapy; Mets: Metastasis; LN: Lymph Nodes; LocRec: Local Recurrence; NED: No Evidence Of Disease; AWD: Alive With Disease; DOD: Dead Of Disease; * excision at 6 months; - : not specified.
References
- F M Enziger F M (1965) Clear cell sarcoma of tendons and aponeuroses. An analysis of 21 cases. Cancer 18: 1163-1174. [Crossref]
- Cristina R Antonescu, Sylvia J Tschernyavsky, James M Woodruff, Achim A Jungbluth, Murray F Brennan et al. (2002) Molecular diagnosis of clear cell sarcoma: detection of EWS-ATF1 and MITF-M transcripts and histopathological and ultrastructural analysis of 12 cases. J Mol Diagn 4: 44-52. [Crossref]
- Wei Lien Wang, Empar Mayordomo, Wenyong Zhang, Vivian S Hernandez, Daniel Tuvin et al. (2009) Detection and characterization of EWSR1/ATF1 and EWSR1/CREB1 chimeric transcripts in clear cell sarcoma (melanoma of soft parts). Mod Pathol 22: 1201-1209. [Crossref]
- G Bianchi, C Charoenlap, S Cocchi, N Rani, S Campagnoni et al. (2014) Clear cell sarcoma of soft tissue: a retrospective review and analysis of 31 cases treated at Istituto Ortopedico Rizzoli. Eur J Surg Oncol 40: 505-510. [Crossref]
- Af Mavrogenis, G Bianchi, Na Stavropoulos, Pj Papagelopoulos, P Ruggieri (2013) Clinicopathological features, diagnosis and treatment of clearcell sarcoma/melanomaof soft parts. Hippokratia 17: 298-302. [Crossref]
- R Yokoyama, K Mukai, T Hirota, Y Beppu, H Fukuma (1996) Primary malignant melanoma (clear cell sarcoma) of bone. Report of a case arising in the ulna. Cancer 77: 2471-2475. [Crossref]
- R K Gelczer, D E Wenger, L E Wold (1999) Primary clear cell sarcoma of bone: a unique site of origin. Skeletal Radiol 28: 240-243. [Crossref]
- Murat Ali Hersekli, Gurkan Ozkoc, Sema Bircan, Sercan Akpinar, Metin Ozalay et al. (2005) Primaryclearcell sarcoma of rib. Skeletal Radiol 34: 167-170. [Crossref]
- Gaetano Rocco, Anna Rosaria de Chiara, Flavio Fazioli, Francesco Scognamiglio, Antonello La Rocca et al. (2009) Primary giant clear cell sarcoma (soft tissue malignant melanoma) of the sternum. Ann Thorac Surg 87: 1927-1928. [Crossref]
- M K Brekke, K Northcote, W E Temple (1998) Clear cell sarcoma in the first metatarsal. An unusual case. J Am Podiatr Med Assoc 88: 457-461. [Crossref]
- J H Choi, M J Gu, M J Kim, Y K Bae, W H Choi et al. (2003) Primary clear cell sarcoma of bone. Skeletal Radiol 32: 598-602. [Crossref]
- Luana Licata, Domenico Fenga, Giuseppe Speciale, Michele Attilio Rosa (2014) Clear cell sarcoma of metatarsus. Folia Med (Plovdiv) 56: 271-274. [Crossref]
- Tsutomu Inaoka, Koji Takahashi, Susumu Tandai, Naoyuki Miyokawa, Yasuyuki Abe et al. (2003) Primary clear cell sarcoma (malignant melanoma) in the right radius. Skeletal Radiol 32: 594-597. [Crossref]
- Constantinos J Kazakos, Vasilios G Galanis, Alexandra Giatromanolaki, Dennis Alexander J Verettas, Efthimios Sivridis (2006) Clear cell sarcoma of the scapula. A case report and review of the literature. World J Surg Oncol 4: 48. [Crossref]
- Xudong Liu, Huizhen Zhang, Yang Dong (2011) Primary clear cell sarcoma of humerus: case report. World J Surg Oncol 9: 163. [Crossref]
- Weibin Zhang, Yuhui Shen, Rong Wan, YanBo Zhu (2011) Primary clear cell sarcoma of the sacrum: a case report. Skeletal Radiol 40: 633-639. [Crossref]
- Shoko Nakayama, Taiji Yokote, Kazuki Iwaki, Toshikazu Akioka, Takuji Miyoshi, et al. (2012) A rare case of primary clear cell sarcoma of the pubic bone resembling small round cell tumor: an unusual morphological variant. BMC Cancer 12: 538. [Crossref]
- Zhe Xu, Haiqiang Suo, Yao Zhang, Wei Feng (2019) Primary clear cell sarcoma of the calcaneus : Report of a rare case and review of the literature. Orthopäde 48: 232-238. [Crossref]
- Marina Pacheco, Douglas E Horsman, Malcolm M Hayes, Paul W Clarkson, Hassan Huwait et al. (2010) Small blue round cell tumor of the interosseous membrane bearing a t(2;22)(q34;q12)/EWS-CREB1 translocation: a case report. Mol Cytogenet 3: 12. [Crossref]