Racemose Pattern of Intracranial Tuberculoma at the Basal, Suprasellar and Perimesencephalic Cisterns – A Case Report
Racemose Pattern of Intracranial Tuberculoma at the Basal, Suprasellar and Perimesencephalic Cisterns – A Case Report
A B S T R A C T
Central nervous system tuberculosis may present as meningitis, tuberculoma, abscesses, cerebritis or miliary tuberculosis. The most common site of tuberculoma has been reported to be at the grey-white matter junction and the periventricular region. They may even be found in the epidural, subdural and subarachnoid spaces, and the brain stem. Although tuberculosis is very common in developing countries, with the increasing prevalence of immunosuppression owing to human immunodeficiency virus and patients surviving chemotherapy or organ transplantation, the incidence of tubercular infections has been rising in developed countries. The authors report a 15-year-old boy of intracranial tuberculoma at the basal, suprasellar and perimesencephalic cisterns in a patient. Tuberculous involvement was noted in a racemose pattern in the subarachnoid space. The patient’s clinical symptoms resolved with no recurrence of symptoms but only persistence of the radiological abnormality after antitubercular chemotherapy.
Keywords
Racemose patterns, tuberculoma, cisterns, antitubercular chemotherapy
Introduction
Central nervous system (CNS) tuberculosis (TB) is a serious form of TB, due to haematogenous spread of Mycobacterium tuberculosis (MT). Clinical central nervous system tuberculosis (CNS TB) involvement comprises three categories: meningitis, intracranial tuberculoma and spinal tuberculous arachnoiditis. CNS TB occurs in approximately 5–10% of all extrapulmonary tuberculosis. Risk factors include young age, immunosuppression, malnutrition, alcoholism and malignancies [1]. Intracranial tuberculomas are the least common presentation of CNS TB, found in 1% of the patients. Multiple lesions are seen in only 15–33% of the cases and mostly in MTB endemic areas. Clinical presentations are seizure, headache, hemiplegia and signs of raised intracranial pressure [2]. Central nervous system tuberculosis is usually secondary to a haematogenous spread from a primary infection. It can sometime present itself in the form of a grape-like cluster of multiple immature tuberculomas, coalescence and caseation of which can result if formation of some of the large mature tuberculomas [3, 4].
Initial stage of CT imaging may show low-dense or iso-dense lesions, while later stage imaging shows encapsulated iso-dense or hypodense lesions with peripheral ring enhancement (target lesions) [3]. Computed tomography (CT) scan is also useful for assessing the presence of cerebral edema, brain stem herniation, and for monitoring the response to medical therapy [5]. Anti-TB drugs are essential for the successful treatment of cerebral tuberculomas and should be initiated based on clinical manifestations and should not be delayed until laboratory confirmation. Treatment of CNS MTB is a four-drug regimen including rifampin, isoniazid, pyrazinamide, and ethambutol (RIPE) or rifampin, isoniazid, pyrazinamide with either fluoroquinolone or aminoglycoside, administered daily for two months. RIPE for 2 months is followed by isoniazid and rifampin for the rest of the course of total 18 months. Ethambutol has poor CNS penetration but can be enhanced with fluoroquinolones. Steroids should be used for the first 6-8 weeks as well [6]. We present a case of tuberculoma involving the subarachnoid spaces in a racemose pattern at the Basal, Suprasellar and Perimesencephalic cisterns which improved after treatment with antitubercular chemotherapy.
Case Report
A 15-year-old boy came to the hospital with a history of gradually progressing left sided weakness of insidious onset for 6 months, low grade intermittent fever for 1 month and generalized headache with early morning exacerbation for 1 month. His physical examination revealed 100° F temperature, early stage papilledema, reduced power of all groups of muscles on the left side (MRC grade 3) with increased tone and exaggerated jerks in the left sided limbs and extensor planter response bilaterally. His gait was hemiplegic. His blood work showed raised ESR (22mm). Sputum for acid fast bacilli was negative. Chest roentgenogram showed a round hyperdensity near the left hilum with mild bilateral hilar patchy opacities (Figure 1).
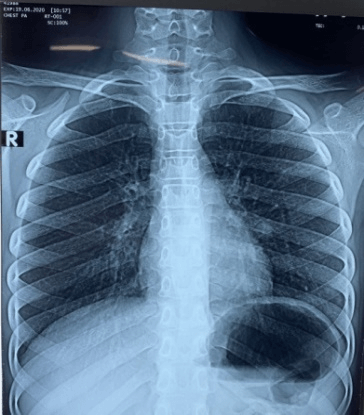
Figure 1: Chest roentgenogram showed a round hyperdensity near the left hilum with mild bilateral hilar patchy opacities.
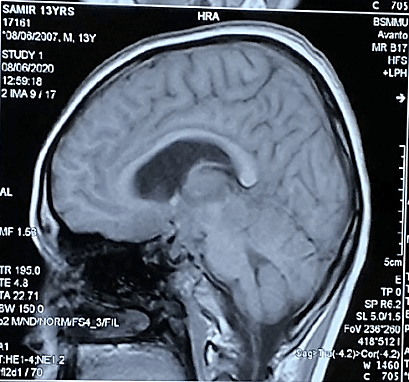
Figure 2: On T1-weighted images showed multiple ill-defined mixed iso to slight hypointensity lesions.
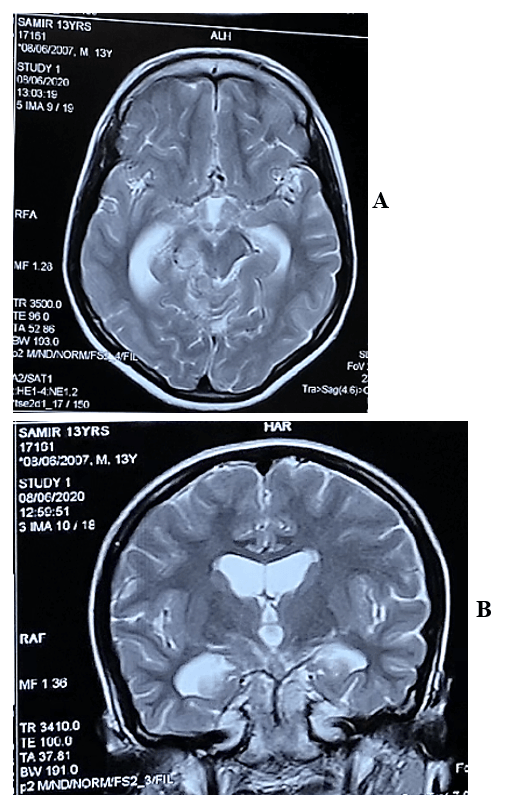
Figure 3: The lesions became heterogeneously hyperintense on T2 WI in A) axial & B) coronal view.
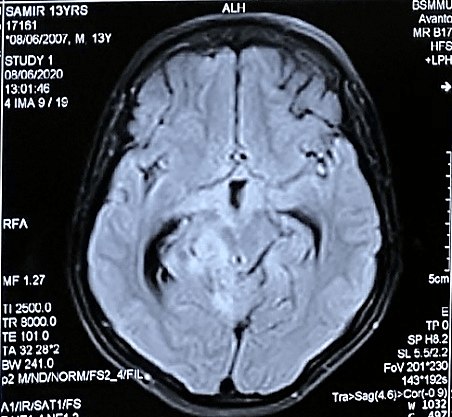
Figure 4: The lesions were also hyperintense in FLAIR images.

Figure 5: After contract enhancement, there were multiple conglomerate ring shaped tuberculomas of 0.5 to 1cm size located at the basal, suprasellar and perimesencephalic cisterns and along the leptomeninges of basal region of cerebral hemisphere with racemose patterns in A) axial & B) sagittal view.
On the MRI T1-weighted images, multiple ill-defined mixed iso to slight hypointensity lesions were found to be located in basal, suprasellar, interpeduncular, prepontine, ambient and quadrigeminal cisterns (Figure 2) and the lesions became heterogeneously hyperintense on T2 WI (Figures 3A & 3B). The lesions were also hyperintense in FLAIR images (Figure 4) and after contract enhancement, there were multiple conglomerate ring shaped tuberculomas of 0.5 to 1cm size located at the basal, suprasellar and perimesencephalic cisterns and along the leptomeninges of basal region of cerebral hemisphere with racemose patterns. The central nonenhancing portions corresponded to caseation necrosis (Figures 5A & 5B). After treatment with antitubercular chemotherapy for 18 months the patient showed complete clinical recovery (Figure 6) but persisting radiological features of tuberculosis.
Figure 6: After treatment with antitubercular chemotherapy the patient showed complete clinical recovery.
Discussion
TB infection occurs through inhalation of a droplet containing bacilli, which leads to the deposition in the lung alveoli and activation of T-helper cells. This T-helper cell immune-mediated response leads to the formation of granuloma and primary pulmonary TB. Prior to the containment of the infection, some bacilli are filtered into the lymphatic system, which leads to hematogenous dissemination to the distant highly oxygenated parts of the body, like the brain. A multitude of factors like host immunity, the virulence of TB strain, and oxygenation plays a vital role in clinical features of TB [2]. The clinical issues regarding CNS tuberculosis vary from mild meningitis with no neurologic deficit to coma. Long-term morbidity occurs in up to 80% and includes mental retardation, paralysis, seizures, rigidity, speech or visual deficits. Pediatric CNS Tuberculosis usually presents as tubercular meningitis with or without hydrocephalus and tuberculomas [4]. In most of the cases, patients had nonspecific findings like headache, fever and weight loss. Altered mental status and focal neurological signs were another common clinical manifestation [7-9]. In this literature review, diagnosis of CNS tuberculoma were mostly based on clinical findings and brain imaging. Similar to our case, AFB stain was helpful to establish the diagnosis [9].
Furthermore, in our case, the patient’s clinical symptoms resolved with no recurrence of symptoms but only persistence of the radiological abnormality. By Pepper et al., the article describes symptomatic resolution in patients at 6 months but the resolution of radiological features was not commented upon [10]. Our case report is unique in its presentation of multiple tuberculomas in the subarachnoid space in a racemose pattern, with involvement of the basal, suprasellar, interpeduncular, prepontine, ambient and quadrigeminal cisterns, which are the rare sites for development of a tuberculoma, while the earlier reported cases have been of parenchymal, optochiasmatic and dural tuberculomas [11]. The pattern of tuberculoma reported as “a racemose pattern” in this report has been seen in a few cases in the literature in basal TBM [11, 12]. However, based on its appearance on images, which was similar to the racemose pattern of neurocysticercosis, the authors refer to this imaging pattern as a racemose pattern of tuberculoma.
Symptoms and radiologic findings of CNS tuberculoma are nonspecific. Therefore, it is a clinically challenging diagnosis. CT scan was reported to have a sensitivity of 100% and specificity of 85.7% in CNS tuberculoma detection. Brain magnetic resonance imaging (MRI) is the technique of choice for further investigation. Lumbar puncture is usually avoided due to the risk for increasing intracranial pressure and brainstem herniation and most of the time findings are nonspecific. Biopsy of the brain lesions is the most accurate method of diagnosis, but it is not essential due to the limitations related to location of the lesions and some associated risks [13]. Investigations usually reveal a raised the erythrocyte sedimentation rate with a positive Mantoux test & PCR. In Plain CT scan of brain tuberculomas are generally isodense but can be hypodense or slightly hyperdense. Calcification is rare (approximately 20%) [14, 15]. In contrast enhanced CT scan these lesions show marked enhancement and can show the following variations - 1. Discs and rings of less than 1cm, 2. A ring of usually 1-2 cm, often with the “target sign” of Welchman which includes central focus of enhancement with ring of peripheral enhancement, 3. Large nodular masses with an irregular outline. Multiple lesions are seen in 15-20% cases [14, 15].
MRI of brain in plain T1-weighted images usually show hypointense lesions in noncaseating granulomas, central hypointensity or isointensity with or without a hyperintensity rim in caseating granulomas. T2-weighted images show hyperintense lesions in noncaseating granulomas, central hypointensity (or hyperintensity if necrotic) sometimes with a hypointense rim in caseating granulomas. There may be signs of surrounding edema. Some tuberculomas have been found to be hyperintense on T1 and hypointense on T2 images. FLAIR images are similar to T2. DWI images may show hyperintense centers. Gadolinium enhanced MRI may show thin nodular, homogeneous enhancement in Noncaseating granulomas and peripheral thin rim enhancement with hypointense necrotic centers in Caseating granulomas. MRS of brain can show a lipid peak on stimulated echo acquisition mode [14].
Nonsurgical treatment with a course of multi-drug antitubercular chemotherapy for 18 months is indicated in all patients with a reasonable suspicion of a tuberculoma, with no imminent threat to vision or life. Steroids can be added if close monitoring of treatment by imaging is possible. Adjunctive corticosteroid treatment provides seizure control and reduces the tuberculoma size and number. Clinical and radiological improvement usually occurs within 2-3 weeks and 4-6 weeks respectively. Stereotactic biopsy can also be done to diagnose any suspected lesion. In life or vision threatening cases surgical treatment is necessary which also confirms the diagnosis in doubtful scenarios [15]. A paradoxical response during the treatment of intracranial tuberculosis is a diagnostic challenge for clinicians and radiologists. Clinicians should be aware of this entity so that anti-tubercular chemotherapy is continued under the cover of corticosteroids [16]. In the reported case, as there was only a minimal change in the size of the tuberculomas, a clinical decision to continue with antitubercular chemotherapy with corticosteroids was taken.
Conclusion
After surveying the literature, we must emphasize the unusual occurrence of CNS TB as a racemose pattern as observed in our case.
Conflicts of Interest
None.
Article Info
Article Type
Case ReportPublication history
Received: Tue 21, Jul 2020Accepted: Fri 31, Jul 2020
Published: Tue 11, Aug 2020
Copyright
© 2023 Saumitra Sarkar. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.08.13
Figures & Tables
References
- Kiran Thakur, Mitashee Das, Kelly E Dooley, Amita Gupta (2018) The global neurological burden of tuberculosis. Semin Neurol 38: 226-237. [Crossref]
- Sreenath Meegada, Richmond Gyamfi, Vijayadershan Muppidi, Vasuki Dandu, Tejo Challa (2020) Multiple Intracranial Tuberculomas with an Intra-medullary Spinal Cord Tuberculoma in a Pediatric Patient. Cureus 12: e7248. [Crossref]
- Christina A Nelson, Joseph R Zunt (2011) Tuberculosis of the central nervous system in immunocompromised patients: HIV infection and solid organ transplant recipients. Clin Infect Dis 53: 915-926. [Crossref]
- Sandip Chatterjee (2011) Brain tuberculomas, tubercular meningitis, and post-tubercular hydrocephalus in children. J Pediatr Neurosci 6: S96-S100. [Crossref]
- Ahmad A Moussa, Mohamed E Mahmoud, Hosam A Yousef (2019) Intracranial tuberculoma and recent advances in magnetic resonance imaging. Egypt J Neurosurg 33: 13.
- E Harder, M Z Al Kawi, P Carney (1983) Intracranial tuberculoma: conservative management. Am J Med 74: 570-576. [Crossref]
- Regina Monteiro, José Carlos Carneiro, Claúdia Costa, Raquel Duarte (2013) Cerebral tuberculomas - A clinical challenge. Respir Med Case Rep 9: 34-37. [Crossref]
- Cicek Bayindir, Ozgür Mete, Bilge Bilgic (2006) Retrospective study of 23 pathologically proven cases of central nervous system tuberculomas. Clin Neurol Neurosurg 108: 353-357. [Crossref]
- A Unal, P N Sutlas (2005) Clinical and radiological features of symptomatic central nervous system tuberculomas. Eur J Neurol 12: 797-804. [Crossref]
- Dominique J Pepper, Suzaan Marais, Gary Maartens, Kevin Rebe, Chelsea Morroni et al. (2009) Neurologic manifestations of paradoxical tuberculosis‐associated immune reconstitution inflammatory syndrome: a case series. Clin Infect Dis 48: e96-e107. [Crossref]
- Parveen K Monga, Upreet Dhaliwal (2009) Paradoxical reaction in tubercular meningitis resulting in involvement of optic radiation. Indian J Ophthalmol 57: 139-141. [Crossref]
- A Pauranik, M Behari, M C Maheshwari (1987) Appearance of tuberculoma during treatment of tuberculous meningitis. Jpn J Med 26: 332-334. [Crossref]
- G Engin, B Acunaş, G Acunaş, M Tunaci (2000) Imaging of extrapulmonary tuberculosis. Radiographics 20: 471-488. [Crossref]
- Miral D Jhaveri, Anne G Osborn, Karen L Salzman, A James Barkovich (2016) Diagnostic imaging: Brain 3rd edn. Philadelphia: Elsevier.
- P N Tandon, R Ramamurthi (2012) Tuberculosis of the Central Nervous System 3rd edn. New Delhi: Jaypee Brothers Medical Publishers.
- M A Whelan, J Stern (1981) Intracranial tuberculoma. Radiology 138: 75-81. [Crossref]