Rare Presentation of Huge Lipoma in the Right Axillary Region in a 10 Months’ Infant
Rare Presentation of Huge Lipoma in the Right Axillary Region in a 10 Months’ Infant
A B S T R A C T
Lipomas are common benign soft tissue tumors which can be seen in many parts of the body, but they are uncommon in axillary region. Axilla is a rare region for lipoma. although lipoma is the most common benign mesenchymal tumor, its location in some regions are uncommon [1]. Moreover, huge and giant lipoma are uncommon. Therefore, axillary giant cell lipoma is rare presentation [2]. Lipomas are seen in subcutaneous tissue of extremities, trunk and neck commonly. Their existence in axillary region is rare. Giant lipoma in adults are 10*10 cm in diameter [3]. Lipomas are originated from mesenchymal fibrofatty tissue. Their usual presentations are soft mass without tenderness which grows slowly [4]. The most common site for location of lipoma is shoulder and back of trunk, and the second common site is head and neck [5]. Lipoma can be seen in GI tract, especially in the colonic wall [6]. Intra osseous primary lipoma is as rare as 0.1% of bone tumors. The most age of such tumor’ s presentation is in 4th decades of life. They are 70% located in the lower extremity [7]. In this case presentation we reported a ten months’ boy who was referred in our hospital due to a large and fast-growing soft tissue mass in his axilla. His arm was in 45-degree angle with the chest wall in upright position of the baby due to the huge mass. The patient was normal in physical examination except a huge and firm mass in right axilla. He had no history of any underlying disease. We found no history of such condition in his family members. Surgical excision of mass was done successfully, and Pathologic findings were mature adipose tissue compatible with lipoma.
Keywords
Lipoma, axillary mass, adipose tissue, infant
Case Presentation
A ten months’ boy was referred in our hospital due to a large and fast-growing soft tissue mass in his axilla. His arm was in 45-degree angle with the chest wall in upright position of the baby due to the huge mass. This mass was observed from 4 months ago. It was as small as peanut at that time and was became bigger during 4 months. The patient was normal in physical examination except a huge and firm mass in right axilla. He had no history of any underlying disease. His weight was 9 kg and vaccination was done completely. We found no history of such condition in his family members. Obstetric history of his mother was without any abnormal condition and he was born in 38 week of gestational age by normal vaginal delivery. His laboratory findings were: WBC=6800, Hgb=11.3, HCT=34.7, PLT=393000, Neutrophil=27.5%, Lymph=65.5%, Mon=5.6%, Eos=1.1%, Baso 0.3%. hypochromia & ovalocyte & target cell was seen.

Figure 1: Magnetic resonance imaging finding of tumor.
In multislice, multiplanar and multisequence MR imaging findings were: T1 & T2 high signal multi lobulated mass lesion with thin internal septa measuring about 70*65*32 mm in right humerus soft tissue without extension to bone. Low signal intensity in fat sat sequence. No evidence of solid enhancement (Figures 1 & 2).

Figure 2: Magnetic resonance imaging finding of tumor.
The patient was prepared for operation under general anaesthesia. We found a large multi lobulated mass which it had light yellow colour and it was firm in palpation. Excision of whole mas was done with saving nerves and vessels saving. (Figures 3 & 4). Pathologic findings were mature adipose tissue compatible with lipoma.
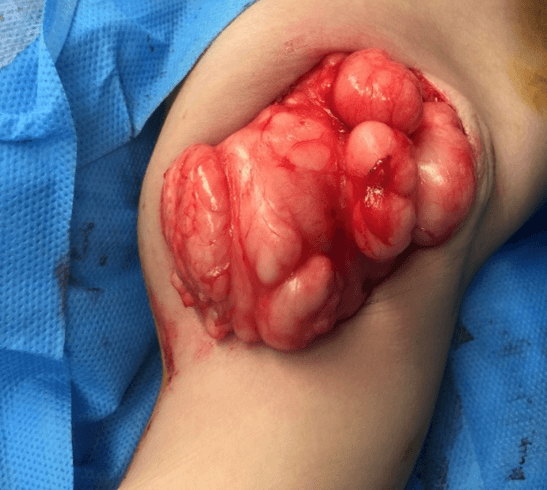
Figure 3: Intra operative photography of the tumor.
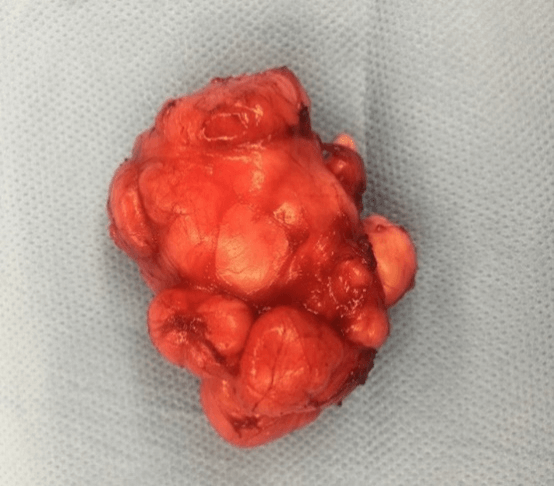
Figure 4: Photography of the tumor after resection.
Discussion
Lipomas are common benign soft tissue tumors which can be seen in many parts of the body, but they are uncommon in axillary region. Axilla is a rare region for lipoma. although lipoma are the most common benign mesenchymal tumor, its location in some regions are uncommon [1]. Moreover, huge and giant lipoma are uncommon. Therefore, axillary giant cell lipoma is rare presentation [2]. Lipomas are seen in subcutaneous tissue of extremities, trunk and neck commonly. Their existence in axillary region is rare. Giant lipoma in adults are 10*10 cm in diameter [3]. Whereas we did not find any definitive size for description of giant lipoma in children, but this size is much smaller than adults. Our patient’s tumor size was 70*65*32 cm which can be a huge tumor in axillary region of a 10 months’ infant. Lipomas are originated from mesenchymal fibrofatty tissue. Their usual presentations are soft mass without tenderness which grows slowly [4].
The most common type of mesenchymal tumor in the body is lipoma. The mucogingival junction of the buccal cavity, palmar region, finger, rectum, intraosseous, axilla are rare sites for presentation of lipoma [1-8]. The most common site for location of lipoma is shoulder and back of trunk, and the second common site is head and neck [5]. Lipoma is seen in 5th & 6th decades of life [5]. Its presentation in infancy is rare specially in the axilla. World Health Organization (WHO) classified soft tissue tumors in 2002. The committee classified these tumors in 9 categories. These 9 categories are: lipoma, lipoblastoma, myolipoma, angiolipoma, lipomatosis, lipomatosis of nerve, spindle cell/pleomorphic lipoma, chondroid lipoma and hibernoma [5]. Lipomas can be confused with other kinds of soft tissue tumors clinically [9].
We can diagnose lipoma by radiological evaluation before surgical excision in 71% of cases [5]. Computed tomography (CT scan) and magnetic resonance imaging (MRI) can be very helpful for diagnosis of these tumors before surgical management [5]. We had done MRI before surgery in our case. Lipoma can be seen in GI tract, especially in the colonic wall. It is usually asymptomatic and become symptomatic when gastrointestinal bleeding, bowel obstruction, invagination, ileus or perforation occurs [6]. Intra osseous primary lipoma is as rare as 0.1% of bone tumors. The most age of such tumor’s presentation is in 4th decades of life. They are 70% located in the lower extremity [7].
However, the axilla is rare site for lipoma, in some articles it is reported in adults. Tenderness is a rare symptom of lipoma, but it is occurred in some cases [2]. Existence of lipoma in pediatrics age group is rare [10]. We did not find any report of huge and giant axillary lipoma in infants. We must consider malignancy in differential diagnosis when large axillary lipoma is seen in clinical evaluation and this diagnosis must be confirmed by pathologic evaluation. The surgical management of lipoma is complete excision because of its well-defined pseudo capsule [3]. Giant axillary lipoma is a challenging problem in surgical management. Surgeon must be familiar to axillary anatomy and deep layers of this region such as axillary artery and axillary vein and their branches. Moreover, axillary nerve plexus saving are very important and challenging in this procedure because of displacement of these organs due to such huge and giant tumor. Specially because of need to complete excision of lipoma for appropriate treatment and recurrence prevention [8].
Article Info
Article Type
Case ReportPublication history
Received: Sat 25, Jul 2020Accepted: Wed 02, Sep 2020
Published: Tue 29, Sep 2020
Copyright
© 2023 Ashjaei Bahar. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JSCR.2020.04.09
Figures & Tables
References
- Gaurav Sharma, Kanu Jain, Archna Nagpal, Chandrababu Sudha Baiju (2016) A rare presentation of lipoma on mandibular mucogingival junction. J Indian Soc Periodontol 20: 199-202. [Crossref]
- Yasuhiro Nakamura, Yukiko Teramoto, Sayuri Sato, Katsuhiro Yamada, Yoshiyuki Nakamura et al. (2014) Axillary giant lipoma: A report of two cases and published work review. J Dermatol 41: 841-844. [Crossref]
- Pattanayak S, Pramanik S (2014) Giant axillary lipoma - A rare case report with review of literature. Hellenic Journal of Surgery 86: 383-385.
- Veena Singh, Vijay Kumar, Arun K Singh (2016) Case report: A rare presentation of Giant palmar lipoma. Int J Surg Case Rep 26: 21-23. [Crossref]
- Efstathios Chronopoulos, Ptohis Nikolaos, Christos Karanikas, Alkis Kalliakmanis, Spyros Plessas et al. (2010) Patient presenting with lipoma of the index finger: a case report. Case J 3: 20. [Crossref]
- Vasileios K Kouritas, Ioannis Baloyiannis, Georgios Koukoulis, Ioannis Mamaloudis, Dimitris Zacharoulis et al. (2011) Spontaneous expulsion from rectum: a rare presentation of intestinal lipomas. World J Emerg Surg 6: 19. [Crossref]
- Samar A Rabbani, Imran Ilyas, Husam Alrumaih (2013) A rare presentation of an intraosseous lipoma in the proximal femur. Am J Case Rep 14: 362-365. [Crossref]
- Lang CL, Andersen CS, Schmidt G, Bonde C (2015) Gigantic subcutaneous lipoma-A case report. JPRAS Open 3: 6-9.
- Araidy S, Joachim M, Shajrawi I, Abu El Naaj I (2018) Rare presentation of mandibular intraosseous cell Lipoma. Oral Maxillofacial Surg Case 4: 166-169.
- Ram Samujh, Nitin James Peters, Ashish Chhabra, Ali Hussein Almudeer (2017) Pleomorphic Lipoma of the Neck in an Infant: A Rare Clinical Entity. J Indian Assoc Pediatr Surg 22: 184-186. [Crossref]