Relationship of Halitosis Concern with Oral Health Behaviors and Knowledge Among Myanmar People
A B S T R A C T
Objective: The objective of this study was to access the relationship of halitosis concern with oral health behaviors and knowledge among Myanmar people.
Methods: This survey was conducted on 257 samples (93 males and 164 females) with the age range from 16 to 65 years old, in Yangon, Myanmar. All the participants filled a questionnaire focusing on halitosis concern, oral health behaviors, and oral health related knowledge. The correlation between halitosis concern and demographic factors, oral health behaviors, and knowledge were analyzed.
Results: 91.8% (n=236) of the sample population with the average age of 32-year-old expressed concern about halitosis, and 65.4% have encountered another person’s bad breath. The participants that reported a concern about halitosis were married people (p<0.05). There is a significant relationship between halitosis concern and oral hygiene practice such as regular toothbrushing, use of toothbrush and toothpaste, less use of any form of tobacco and high oral health knowledge (p<0.05).
Conclusion: This study showed that a person who concerns halitosis had better oral hygiene behaviors and oral health knowledge than those who do not a concern. The prevalence of halitosis concern was high, and there is a need to recommend taking proper halitosis measurements by professionals and to improve public knowledge about halitosis. It is essential to support best practices and empowerment for effective self-care.
Keywords
Halitosis concern, oral hygiene practices, behaviors, myanmar
Introduction
Halitosis comes from the Latin word “halitus” (breath) and Greek “osis” (pathological process), to describe a condition of unpleasant smells from the mouth. Other names used are bad breath, breath malodor, oral malodor, fetor ex ore, fetor-oris etc. [1]. There are many studies have been conducted about halitosis in various communities, and according to these studies, the oral cavity origin is the main source of halitosis attributed to almost 90% of the cases [2-5]. The reason for that includes severe dental and periodontal diseases, poor oral hygiene practices, stagnation of food debris especially on the dorsum of the tongue, etc. [1, 4, 6-8]. Additionally, individual oral hygiene practices and lifestyle behaviors (including betel quid chewing, smoking and alcohol drinking) are also responsible for halitosis [1]. According to the self-perceived halitosis study among dental patients in Myanmar reported that person with self-perceived halitosis were more likely to chew betel quid and tobacco smoking [9].
Health behavior influences the variation of disease processes among people who are exposed to relatively similar risk factors for disease. An individual’s health concern is one of the influencing factors on a person’s health related behaviors. Nowadays, peoples’ awareness on halitosis (bad breath) is increasing. It is difficult to notice one’s own bad breath, and a person’s bad breath undeniably irritates to other people. Halitosis is highly negative impacts on an individual’s daily life activities, self-esteem, social isolation, self-consciousness, even in suicide attempts [10, 11]. Oral breath can be improved by proper self-oral hygiene practices such as appropriate and efficient tooth brushing, using mouthwashes and tongue cleaning [12]. Professional guidance with appropriate management and oral-prophylaxis is also important to relieve a patient’s suffering of oral bad breath [13].
Concerning on halitosis triggers an individual’s oral healthcare behavioral such as more awareness on self-oral healthcare, seeking health related information and professional care, avoiding risk factors such as tobacco and alcohol use etc. The previous study proved that participants who had stronger health concerns showed healthy behaviors and better health status [14]. A study have been conducted in Nigeria also reported that people who concern about halitosis had better oral self-care practices such as tooth brushing frequency, mouthwash, and dental floss use etc. [15]. Therefore, it is expected that people concern on their oral health status would be an important part of an individual’s health behaviors and seeking professional healthcare. The objective of this study was to access the relationship of halitosis concern with oral health practice, behaviors and knowledge among Myanmar people.
Material and methods
A structured questionnaire survey was conducted on a convenience sample of 257 (93 males and 164 females) with the age range from 16 to 65 years old, in Yangon, Myanmar. As it is the “Questionnaire Survey” focusing on halitosis concern, oral health behaviors, and oral health related knowledge was filled by all participants. All the participants in the study were voluntary. The purpose of the study was explained to the participants, and informed consent was obtained before the onset of the study. A self-completed questionnaire collected socio-demographic information (such as age, gender, and education level), the experience of health education, self-perceived oral health status, knowledge of oral health (7 questions) and an individual’s halitosis concern “Do you worry about having oral bad breath”. Questions on oral health knowledge and behaviors were collected based on Azodo C et al. study [15]. An oral health knowledge score was calculated by simply adding the number of correctly answered questions ranging from 0 to 7.
The analysis was performed using statistical packages for the social science version 20. Characteristics of the participants are presented as descriptive statistics like frequencies and percentages. The correlation between halitosis concern with socio-demographics, oral health behaviors, and knowledge was analyzed by the chi-squared test. Additionally, the relationship of halitosis concern (yes or no) with self-perceived oral health status and the experience of health education was also examined. The findings are presented in tables and graph form. The study protocol was authorized by the University of Dental Medicine (Yangon) and approved by the ethical committee of Tokyo Medical and Dental University, Japan (No. 850).
Results
Among a total of 257 participants, 63.8% (n=164) were female and the rest are male participants with the age range from 16 to 65 years old. 91.8% (n=236) of the sample population with the average age of 32-year-old expressed concern about halitosis, and 65.4% have encountered another person’s bad breath. Nearly 40% of the sample responded that another person’s bad breath irritated their daily routine. Almost half of the study participants had no health education experience. The samples’ characteristics and the experience of halitosis were shown in (Table 1). The relationship of halitosis concern with socio-demographics, health education experiences, and self-perceived oral health status was reported in (Table 2). Halitosis concern was significantly higher in aged 35 years old and under, and married people. Although there is no significant relationship, a high proportion of halitosis concerned was seen in high education level group, participants with no experience in health education and individual with poor self-perceived oral health status.
Table 1: Sample characteristics and experienced on halitosis.
|
Variable |
N |
% |
|
Age |
||
|
35 years and under |
160 |
62.3 |
|
over 35 years |
97 |
37.7 |
|
Gender |
||
|
Male |
93 |
36.2 |
|
Female |
164 |
63.8 |
|
Marital status |
||
|
Single |
97 |
37.7 |
|
Married |
160 |
62.3 |
|
Education level |
||
|
Until middle school finished |
68 |
26.5 |
|
High school and above |
189 |
73.5 |
|
Health education experience |
||
|
Present |
124 |
48.2 |
|
Absent |
133 |
51.8 |
|
Self-perceived oral health status |
||
|
Good |
199 |
77.4 |
|
Poor |
58 |
22.6 |
|
Halitosis concern |
||
|
Yes |
236 |
91.8 |
|
No |
21 |
8.2 |
|
Halitosis effect on daily activities |
||
|
Agree |
244 |
94.9 |
|
Disagree |
13 |
5.1 |
|
Encountered another person with bad breath |
||
|
Yes |
168 |
65.4 |
|
No |
89 |
34.6 |
|
Annoying daily routine because of other person's bad breath |
||
|
Yes |
102 |
39.7 |
|
No |
155 |
60.3 |
Mean oral health related knowledge score in the group who concerned halitosis and who did not were significantly different, with 4.13±1.56 and 2.62± 1.63, respectively (p<0.001). The mean knowledge score (4.60±1.44) in the group with health education experiences was significantly higher (p<0.001) than its counterpart group with the mean score of 3.45±1.57. Relationship of halitosis concern with individual question on oral health knowledge was shown in (Table 3). Participants who concerned halitosis responded more correct answers than their counterpart and they had high oral health knowledge. There is a significant relationship between halitosis concern and oral health related behaviors shown in (Figure 1). The participants who concerned about halitosis had significantly more regularly tooth brushing, use of toothbrush and toothpaste, less use of any form of tobacco than the person who did not a concern (p<0.05).
Table 2: Relationship of halitosis concern with socio-demographics, health education experience, and self-perceived oral health status.
|
Variables |
Concern Halitosis |
P-value |
|||||
|
Yes (n=236) |
No (n=21) |
Total (n=257) |
|||||
|
N |
Row % |
N |
Row % |
N |
% |
||
|
Age |
|||||||
|
35 years and under |
152 |
95.0 |
8 |
5.0 |
160 |
100 |
0.017 |
|
over 35 years |
84 |
86.6 |
13 |
13.4 |
97 |
100 |
|
|
Gender |
|||||||
|
Male |
83 |
89.2 |
10 |
10.8 |
93 |
100 |
0.255 |
|
Female |
153 |
93.3 |
11 |
6.7 |
164 |
100 |
|
|
Marital status |
|||||||
|
Single |
84 |
86.6 |
13 |
13.4 |
97 |
100 |
0.017 |
|
Married |
152 |
95.0 |
8 |
5.0 |
160 |
100 |
|
|
Education level |
|||||||
|
Until middle school finished |
59 |
86.8 |
9 |
13.2 |
68 |
100 |
0.075 |
|
High school and above |
177 |
93.7 |
12 |
6.3 |
189 |
100 |
|
|
Health education experience |
|||||||
|
Present |
118 |
88.7 |
15 |
11.3 |
133 |
100 |
0.060 |
|
Absent |
118 |
95.2 |
6 |
4.8 |
124 |
100 |
|
|
Self-perceived oral health status |
|||||||
|
Good |
181 |
91.0 |
18 |
9.0 |
199 |
100 |
0.343 |
|
Bad |
55 |
94.8 |
3 |
5.2 |
58 |
100 |
|
Table 3: Relationship of halitosis concern with oral health knowledge.
|
Variables |
Halitosis concern |
P-value |
|||||
|
Yes (n=236) |
No (n=21) |
Total (n=257) |
|||||
|
N |
% |
N |
% |
N |
% |
||
|
Tooth decay is preventable. |
|||||||
|
Yes |
194 |
82.2 |
16 |
76.2 |
210 |
100 |
0.495 |
|
No |
42 |
17.8 |
5 |
23.8 |
47 |
100 |
|
|
Gum bleeding is a sign of gingivitis. |
|
|
|||||
|
Yes |
153 |
64.8 |
9 |
42.9 |
162 |
100 |
0.046 |
|
No |
8 |
35.2 |
12 |
57.1 |
95 |
100 |
|
|
Gingivitis is preventable. |
|
|
|||||
|
Yes |
123 |
52.1 |
7 |
33.3 |
130 |
100 |
0.099 |
|
No |
113 |
47.9 |
14 |
66.7 |
127 |
100 |
|
|
Plaque is the soft deposit of food on the tooth surface. |
|
|
|||||
|
Yes |
124 |
52.5 |
5 |
23.8 |
129 |
100 |
0.012 |
|
No |
112 |
47.5 |
16 |
76.2 |
128 |
100 |
|
|
Fluoride is effective against caries. |
|
|
|||||
|
Yes |
119 |
50.4 |
4 |
19.0 |
123 |
100 |
0.006 |
|
No |
117 |
49.6 |
17 |
81.0 |
134 |
100 |
|
|
Oral Health is related to general health |
|
|
|||||
|
Yes |
185 |
78.4 |
11 |
52.4 |
196 |
100 |
0.007 |
|
No |
51 |
21.6 |
10 |
47.6 |
61 |
100 |
|
|
Tongue coating is related with halitosis |
|
|
|||||
|
Yes |
77 |
32.6 |
3 |
14.3 |
80 |
100 |
0.082 |
|
No |
159 |
67.4 |
18 |
85.7 |
177 |
100 |
|
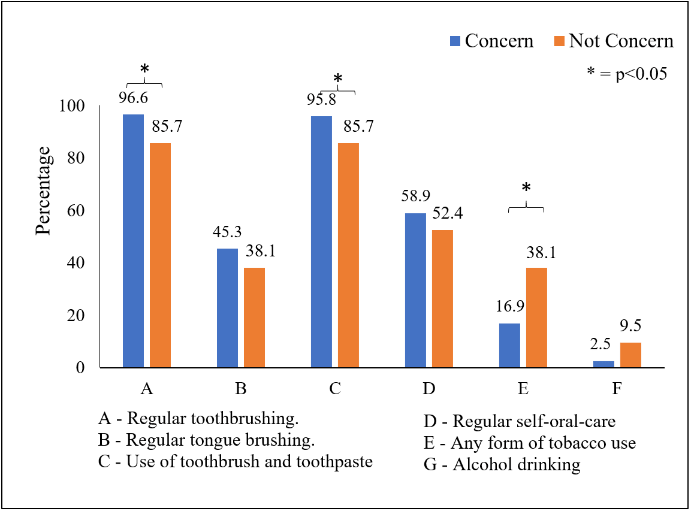
Figure 1: Relationship between halitosis concern and oral health related behaviors.
Discussion
Concern about halitosis is rising nowadays, and it is the main reason for dentist consultation. Halitosis is a major concern for embracement and even leads to social loneliness and an attempt to commit suicide [10, 16]. In this study, the proportion of respondents who concerned halitosis was so high (91.8%). A study on halitosis concern on Nigeria reported that more than half of the participants expressed concern about halitosis [15]. And also, results from the current study is higher than the study among the high schools’ male students in Tokyo with 55.4%, 40% in Brazil high school students, 66.3% in among Indian dental students and 78% in Jordanian population [2, 17-19]. The differences between nations regarding the halitosis concern might be influenced by culture and sample populations. The reason for high halitosis concerns in the study’s participants might be due to their experiences of halitosis from other people. 65.4% of the subjects in this study encountered another person with bad breath. The previous study on dental patients in Myanmar stated that 40% of the subjects had a self-perceived oral malodor [9]. The data from this study showed that halitosis concern was higher than self-reported halitosis among dental patients, in Myanmar.
In this study, although there is no significant relationship, halitosis concern was higher among females and a person with a high education level. A person who is married had a significant concern about halitosis than single. These findings are the same with previous studies where concern about halitosis was higher among females than males, married and higher education associated [11, 15]. And also, this study presented that halitosis concern was higher in the aged 35 years-old and under. It is due to the awareness of psychosocial impact resulting in a negative impression on dating, poor social communication in daily life, personal anxiety, a decrease in social activity involvement and embarrassment [20, 21].
Oral health knowledge score is related to health education experiences in this study. This finding is absolutely due to the effect of health education, where experiences of health education get a higher level of related knowledge than in those without experiences. Moreover, lower oral health knowledge score was seen in the participants who did not concern about halitosis than who did concern. Higher concern of halitosis might be due to the increased awareness of oral health and motivated to find health-related information. Regarding the health behavior, respondents in the group of concern about halitosis have brushed their teeth more regularly than respondents who did not a concern and also have brushed their teeth by using a toothbrush and toothpaste. Although there is no significant difference between groups, tongue cleaning behavior is more practiced in the group of halitosis concerns. In addition, people who concern halitosis do more regular oral checkups by themselves.
A lower proportion of the study population who reported a concern about halitosis had tobacco usage and alcohol drinking behavior. This finding is the same as the previous study in which participants expressed halitosis concerns had poor oral hygiene practices and behaviors like alcohol drinking, smoking [15]. Therefore, the study results showed that if the person concern about halitosis, he/she would be more focused on self-oral-healthcare practices to reduce their anxiety on it than those who did not a concern. As there are differences between concern about halitosis and self-perceived halitosis, many studies reported that a person with poor oral hygiene practice and behaviors is significantly linked with self-perceived halitosis [9, 22]. This study showed that people’ health concern is strongly related to their health-related behaviors, practices and also motivates to learn more about related health knowledge. There are some limitations to this study. As this study was conducted in Yangon region, it is needed to be a caution to represent as a nation-wide. Additionally, this study mainly focuses on the halitosis concern and clinical halitosis evaluation was not performed. Nevertheless, this study would give some information in considering changing people’s behaviors related to oral health in Myanmar and be a great help to implement appropriate oral health promotion programs.
Conclusion
This study showed that a person who concerned halitosis had better oral hygiene practices, behaviors and a high level of oral health knowledge than those who did not a concern. It can be concluded that concern about halitosis triggered the participants’ good oral hygiene practices. As the prevalence of halitosis concern was high in this study, it is necessary to recommend taking proper halitosis measurements by professionals and to improve public knowledge about halitosis. Moreover, it is essential to support best practices and empowerment for effective self-care on individual oral health.
Conflicts of Interest
The authors declare that they have no competing interests.
Article Info
Article Type
Research ArticlePublication history
Received: Fri 30, Aug 2019Accepted: Mon 16, Sep 2019
Published: Tue 01, Oct 2019
Copyright
© 2023 Ei Ei Aung. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JDOA.2019.01.03
Figures & Tables
Table 1: Sample characteristics and experienced on halitosis.
|
Variable |
N |
% |
|
Age |
||
|
35 years and under |
160 |
62.3 |
|
over 35 years |
97 |
37.7 |
|
Gender |
||
|
Male |
93 |
36.2 |
|
Female |
164 |
63.8 |
|
Marital status |
||
|
Single |
97 |
37.7 |
|
Married |
160 |
62.3 |
|
Education level |
||
|
Until middle school finished |
68 |
26.5 |
|
High school and above |
189 |
73.5 |
|
Health education experience |
||
|
Present |
124 |
48.2 |
|
Absent |
133 |
51.8 |
|
Self-perceived oral health status |
||
|
Good |
199 |
77.4 |
|
Poor |
58 |
22.6 |
|
Halitosis concern |
||
|
Yes |
236 |
91.8 |
|
No |
21 |
8.2 |
|
Halitosis effect on daily activities |
||
|
Agree |
244 |
94.9 |
|
Disagree |
13 |
5.1 |
|
Encountered another person with bad breath |
||
|
Yes |
168 |
65.4 |
|
No |
89 |
34.6 |
|
Annoying daily routine because of other person's bad breath |
||
|
Yes |
102 |
39.7 |
|
No |
155 |
60.3 |
Table 2: Relationship of halitosis concern with socio-demographics, health education experience, and self-perceived oral health status.
|
Variables |
Concern Halitosis |
P-value |
|||||
|
Yes (n=236) |
No (n=21) |
Total (n=257) |
|||||
|
N |
Row % |
N |
Row % |
N |
% |
||
|
Age |
|||||||
|
35 years and under |
152 |
95.0 |
8 |
5.0 |
160 |
100 |
0.017 |
|
over 35 years |
84 |
86.6 |
13 |
13.4 |
97 |
100 |
|
|
Gender |
|||||||
|
Male |
83 |
89.2 |
10 |
10.8 |
93 |
100 |
0.255 |
|
Female |
153 |
93.3 |
11 |
6.7 |
164 |
100 |
|
|
Marital status |
|||||||
|
Single |
84 |
86.6 |
13 |
13.4 |
97 |
100 |
0.017 |
|
Married |
152 |
95.0 |
8 |
5.0 |
160 |
100 |
|
|
Education level |
|||||||
|
Until middle school finished |
59 |
86.8 |
9 |
13.2 |
68 |
100 |
0.075 |
|
High school and above |
177 |
93.7 |
12 |
6.3 |
189 |
100 |
|
|
Health education experience |
|||||||
|
Present |
118 |
88.7 |
15 |
11.3 |
133 |
100 |
0.060 |
|
Absent |
118 |
95.2 |
6 |
4.8 |
124 |
100 |
|
|
Self-perceived oral health status |
|||||||
|
Good |
181 |
91.0 |
18 |
9.0 |
199 |
100 |
0.343 |
|
Bad |
55 |
94.8 |
3 |
5.2 |
58 |
100 |
|
Table 3: Relationship of halitosis concern with oral health knowledge.
|
Variables |
Halitosis concern |
P-value |
|||||
|
Yes (n=236) |
No (n=21) |
Total (n=257) |
|||||
|
N |
% |
N |
% |
N |
% |
||
|
Tooth decay is preventable. |
|||||||
|
Yes |
194 |
82.2 |
16 |
76.2 |
210 |
100 |
0.495 |
|
No |
42 |
17.8 |
5 |
23.8 |
47 |
100 |
|
|
Gum bleeding is a sign of gingivitis. |
|
|
|||||
|
Yes |
153 |
64.8 |
9 |
42.9 |
162 |
100 |
0.046 |
|
No |
8 |
35.2 |
12 |
57.1 |
95 |
100 |
|
|
Gingivitis is preventable. |
|
|
|||||
|
Yes |
123 |
52.1 |
7 |
33.3 |
130 |
100 |
0.099 |
|
No |
113 |
47.9 |
14 |
66.7 |
127 |
100 |
|
|
Plaque is the soft deposit of food on the tooth surface. |
|
|
|||||
|
Yes |
124 |
52.5 |
5 |
23.8 |
129 |
100 |
0.012 |
|
No |
112 |
47.5 |
16 |
76.2 |
128 |
100 |
|
|
Fluoride is effective against caries. |
|
|
|||||
|
Yes |
119 |
50.4 |
4 |
19.0 |
123 |
100 |
0.006 |
|
No |
117 |
49.6 |
17 |
81.0 |
134 |
100 |
|
|
Oral Health is related to general health |
|
|
|||||
|
Yes |
185 |
78.4 |
11 |
52.4 |
196 |
100 |
0.007 |
|
No |
51 |
21.6 |
10 |
47.6 |
61 |
100 |
|
|
Tongue coating is related with halitosis |
|
|
|||||
|
Yes |
77 |
32.6 |
3 |
14.3 |
80 |
100 |
0.082 |
|
No |
159 |
67.4 |
18 |
85.7 |
177 |
100 |
|
References
- Tungare S, Paranjpe AG (2019) Halitosis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. [Crossref]
- Yokoyama S, Ohnuki M, Shinada K, Ueno M, Clive Wright FA et al. (2010) Oral malodor and related factors in Japanese senior high school students. J Sch Health 80: 346-352. [Crossref]
- Rayman S, Almas K (2008) Halitosis among racially diverse populations: an update. Int J Dent Hyg 6: 2-7. [Crossref]
- De Geest S, Laleman I, Teughels W, Dekeyser C, Quirynen M (2016) Periodontal diseases as a source of halitosis: a review of the evidence and treatment approaches for dentists and dental hygienists. Periodontol 2000 71: 213-227. [Crossref]
- Quirynen M, Dadamio J, Van den Velde S, De Smit M, Dekeyser C et al. (2009) Characteristics of 2000 patients who visited a halitosis clinic. J Clin Periodontol 36: 970-975. [Crossref]
- Cortelli JR, Barbosa MDS, Westphal MA (2008) Halitosis: a review of associated factors and therapeutic approach. Braz Oral Res 22: 44-54. [Crossref]
- Rösing CK, Loesche W (2011) Halitosis: an overview of epidemiology, etiology and clinical management. Braz Oral Res 25: 466-471. [Crossref]
- Zurcher A, Filippi A (2012) Findings, diagnoses and results of a halitosis clinic over a seven-year period. Schweiz Monatsschr Zahnmed 122: 205-216. [Crossref]
- Aung EE, Zaitsu T, Ueno M, Kawaguchi Y (2015) Relationship of oral health knowledge, behavior and status with selfperceived and clinical oral malodor among dental patients. J Dent Health Oral Disord Ther 3: 83.
- Sharma S, Shankar T, Koirala B (2011) Halitosis: a serious social problem. Health Renaissance 9: 106-111.
- Vali A, Roohafza H, Keshteli AH, Afghari P, Javad Shirani M et al. (2015) Relationship between subjective halitosis and psychological factors. Int Dent J 65: 120-126. [Crossref]
- Aung EE, Ueno M, Zaitsu T, Furukawa S, Kawaguchi Y (2015) Effectiveness of three oral hygiene regimens on oral malodor reduction: a randomized clinical trial. Trials 16 :31. [Crossref]
- Bicak DA (2018) A current approach to halitosis and oral malodor-A mini review. Open Dent Journal 12: 322-330. [Crossref]
- Hsu W, Chiang C, Yang S (2014) The effect of individual factors on health behaviors among college students: the mediating effects of eHealth literacy. J Med Internet Res 16: e287. [Crossref]
- Azodo CC, Onyeagba MI, Odai CD (2011) Does concern about halitosis influence individual's oral hygiene practices? Niger Med 52: 254. [Crossref]
- Troger B, Almeida Jr HLd, Duquia RP (2014) Emotional impact of halitosis. Trend Psychiat psychother 36: 219-221.
- Lopes MH, Rösing CK, Colussi PR, Muniz FW, Linden MS (2016) Prevalence of self-reported halitosis and associated factors in adolescents from Southern Brazil. Acta Odontol Latinoam 29: 93-103. [Crossref]
- Dagli RJ, Tadakamadla S, Dhanni C, Duraiswamy P, Kulkarni S (2008) Self reported dental health attitude and behavior of dental students in India. J Oral Sci 50: 267-272. [Crossref]
- Hammad MM, Darwazeh AM, Al-Waeli H, Tarakji B, Alhadithy TT (2014) Prevalence and awareness of halitosis in a sample of Jordanian population. J Int Soc Prev Community Dent 4: S178-S186. [Crossref]
- Azodo C, Osazuwa-Peters N, Omili M (2010) Psychological and social impacts of halitosis: A review. J Social Psychol Sci 3: 74-92.
- Settineri S, Mento C, Gugliotta SC, Saitta A, Terranova A et al. (2010) Self-reported halitosis and emotional state: impact on oral conditions and treatments. Health Qual Life Outcomes 8: 34. [Crossref]
- Setia S, Pannu P, Gambhir RS, Galhotra V, Ahluwalia P, et al. (2014) Correlation of oral hygiene practices, smoking and oral health conditions with self perceived halitosis amongst undergraduate dental students. J Nat Sc Biol Med 5: 67-72. [Crossref]