Journals
Remote Endarterectomy for an Occluded Superficial Femoral Artery (SFA) Stent – a Hybrid Technique for the SFA Intervention Toolbox
A B S T R A C T
Remote SFA endarterectomy is a hybrid technique that affords lower limb revascularization without the patient having to undergo a bypass operation especially when the vessels are small (women, Asian decent) and the run off poor. The procedure allows for a larger calibre SFA lumen to be gained, which cannot be obtained from a repeat endovascular procedure for in stent occlusion. Remote endarterectomy down to infrageniculate level has not been previously reported. We describe a modified version of remote endarterectomy with use of a subintimal wire to help remove an occluded SFA stent in the setting of a calcified SFA. This hybrid technique is ideal for flush SFA occlusions.
Keywords
Remote, superficial femoral artery, hybrid, endarterectomy
Background
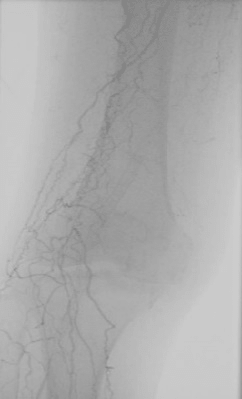
Remote superficial femoral artery (SFA) endarterectomy is a hybrid treatment option for long flush SFA occlusions. We describe a modified version of this technique to remove an occluded SFA stent in a patient who presented with a non-healing forefoot amputation wound and rest pain with severe multi-level disease and single vessel peroneal runoff (Figure 1).
Hybrid Technique
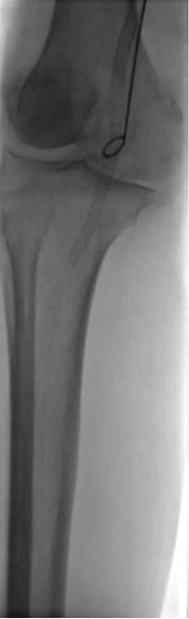
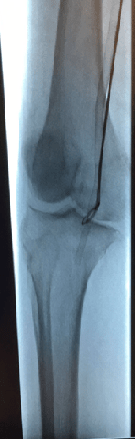
The patient is positioned supine with the ipsilateral buttock propped up. With hyperextension at the hip joint, this allows more space for maneuvering of the Vollmar ring dissector (LeMaitre, Massachusetts, USA) and Mollring cutter. A longitudinal groin incision is made and the common femoral artery (CFA), SFA and profunda femoris artery (PFA) are dissected out and slung. A diagnostic angiogram is performed via a micropuncture sheath inserted retrogradely into the CFA (Figure 2a &b) to discern the extent of subsequent dissection down the SFA with the Vollmar ring dissector. The puncture site is closed, intravenous heparin administered, and the proximal arterial clamp is placed just distal to the PFA. A longitudinal SFA arteriotomy is made such that the atheromatous core is circumferentially dissected from the adventitia using a Penfield elevator for a good 3cm distally and is transected proximally. A Vollmar ring dissector is passed through the distal portion of the atheromatous core and dissection begins under fluoroscopic guidance (Figure 3a). This is the difficult aspect of the procedure as the plane between the stent and wall will be scarred, especially if the arterial wall is also calcified. We have used an angled 0.035” Terumo Glidewire (Terumo Interventional Systems, New Jersey, USA) wire and Bernstein II support catheter (Boston Scientific, Massachusetts, USA) to help with the subintimal dissection process prior to reintroducing Vollmar ring to move down over it and avoid perforation (Figure 3b). The dissection stops at the level of the tibioperoneal trunk, below the stent. The Vollmar Ring dissector is removed and a Mollring cutter of an appropriate size (usually one size bigger than the dissector used) (Figure 3c) is introduced down the dissected plane and the lesion is then cut at the appropriate level [1]. The long strip of stent and atheromatous plaque are removed en-bloc (Figure 4). The SFA arteriotomy may be extended into the CFA. The terumo wire is kept in situ whilst a patch angioplasty is performed next, to allow forward blood flow before the distal flap is tacked down with a bare metal stent (Figure 5a & b).
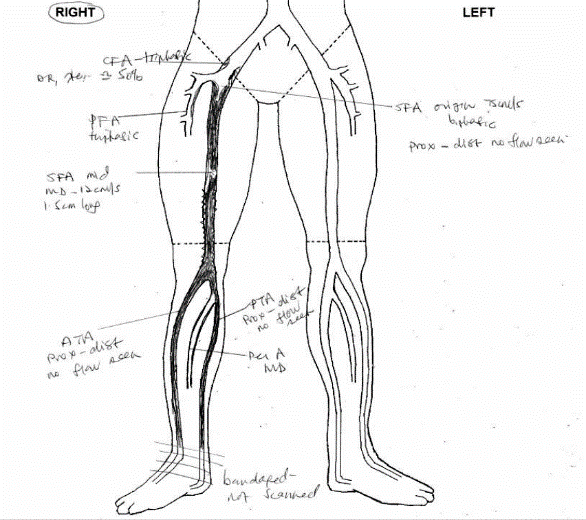
Figure 1: Pre-operative duplex arterial scan showing occluded stent and single vessel run-off via peroneal artery
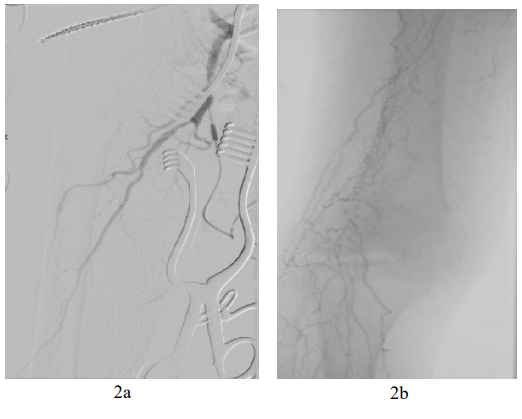
Figure 2a: Initial angiogram showing occlusion of SFA from origin
Figure 2b: Occlusion of distal SFA with collateral circulation
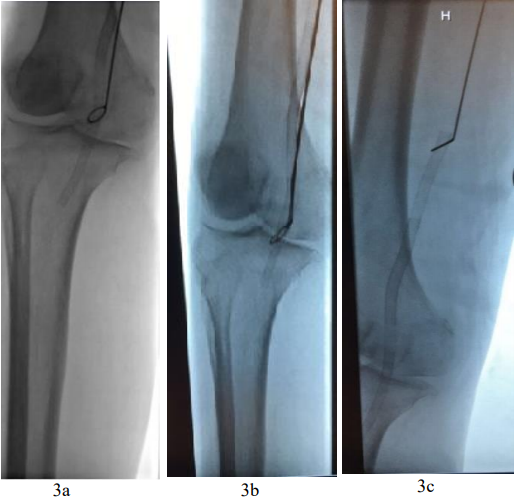
Figure 3a: Vollmar ring dissector being passed down to below the stent
Figure 3b: Vollmar ring over terumo wire/ber II catheter as a lead
Figure 3c: Mollring cutter being introduced down into the dissected plane
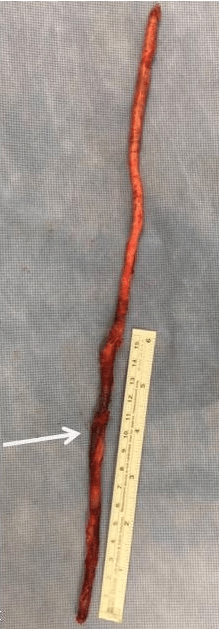
Figure 4: Long strip of atheromatous plaque removed en-bloc with stent, arrow indicating location of stent
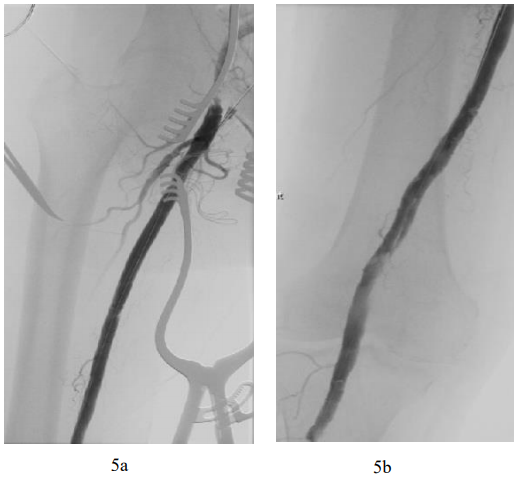
Figure 5a: Final angiogram showing reperfusion of SFA from origin
Figure 5b: Final angiogram showing reperfusion of distal SFA
Discussion
Remote SFA endarterectomy is a hybrid technique that affords lower limb revascularization without the patient having to undergo a bypass operation especially when the vessels are small (women, Asian decent) and the run off poor. The procedure allows for a larger calibre SFA lumen to be gained, which cannot be obtained from a repeat endovascular procedure for in stent occlusion. Remote endarterectomy down to infrageniculate level has not been previously reported. Using a Terumo wire with Berenstein II catheter to assist the subintimal dissection is a useful technique, especially for calcified vessels whereby risk of perforation and inability to move the Vollmar ring dissector forward down the subintimal plane is high.
Declaration of Competing Interests
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article
Funding
The authors received no financial support to conduct this research.
Article Info
Article Type
Case ReportPublication history
Received: Thu 28, Feb 2019Accepted: Fri 22, Mar 2019
Published: Fri 03, May 2019
Copyright
© 2023 Tjun Yip Tang . This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2019.02.016
Author Info
Corresponding Author
Tjun Yip TangDepartment of Vascular Surgery, Singapore General Hospital, Singapore
Figures & Tables




References
- GH Ho, FL Moll, PP Joosten, ED van de Pavoordt, TT.
The Mollring Cutter remote endarterectomy: preliminary experience with a new endovascular technique for treatment of occlusive superficial femoral artery disease J Endovasc Surg, 2 (1995), pp. 278-287