Reusable Vessel Sealing Device Can Significantly Reduce Medical Costs Compared to Disposable Device in Modified Total Neck Dissection
A B S T R A C T
Vessel sealing devices have been described to be effective, allowing to perform procedures with reduced blood loss and shorter operative times in head and neck surgery. Since the traditional vessel sealing devices are all disposable and expensive, there are not often used even in advanced cancer surgery in terms of cost. On the other hand, ‘marClampCut IQ’ (KLS Martin, Tuttlingen, Germany) is a new reusable vessel sealing device. In this clinical study, a traditional disposable device ‘LigaSure small jaw’ and a reusable device ‘marClampCut IQ’ were particularly compared regarding medical expenses and efficacy in modified total neck dissection. Between October 2014 and April 2020, modified total neck dissections were performed using the ‘LigaSure small jaw’ for 56 patients aged from 26y/o to 88y/o (median:66.0y/o). The ‘marClampCut IQ’ was mainly used between November 2018 and April 2020 for 64 modified total neck dissections in patients aged from 31y/o to 91y/o (median:70.5y/o). The amount of blood loss was significantly more in the ‘LigaSure small jaw’ group than in the ‘marClampCut IQ’ group (U-test, P = 0.006). There were no significant differences in age and operation time between the ‘LigaSure small jaw’ group and the ‘marClampCut IQ’ group. When calculated based on the list price in Japan, ‘LigaSure small jaw’ costed $1,000 each; on the other hand, ‘marClampCut IQ’ costed $240 per operation. We found that we could save $760 per operation using ‘marClampCut IQ’. The new reusable device ‘marClampCut IQ’ provided similar clinical efficacy and safety with a highly reduced cost when compared to the disposable device ‘LigaSure small jaw’ in this clinical study of modified total neck dissection.
Keywords
Vessel sealing, reusable device, cost, blood loss, neck dissection
Introduction
Recently, many surgical devices have been developed in keeping with the increase of technical requirements in complicated surgical techniques. Especially for electrosurgery, the surgical devices are complex and diverse. It would be strongly believed that these new technologies should be innovated for safe surgical treatment and easy handling, which would lead to the utmost efficiency in surgical units.
For example, one of the latest bipolar vessel sealing tools is effective for hemostasis, which leads to the reduction of blood loss and operative time. A type of bipolar electrothermal coagulation device, LigaSure Vessel Sealing System (Covidien Valleylab, Boulder, CO, USA) has been developed as a safer and more effective technology for surgical treatment compared to monopolar electric knives (Figure 1). The new device consists of forceps and bipolar radiofrequency generator, which exhibits a wide range of precisely regulated currents and enables surgeons to choose a great number of applications, such as monopolar/bipolar cutting and coagulation modes. It has already been widely used in various surgical procedures, not only for craniofacial surgery but also for abdominal surgery [1-8].
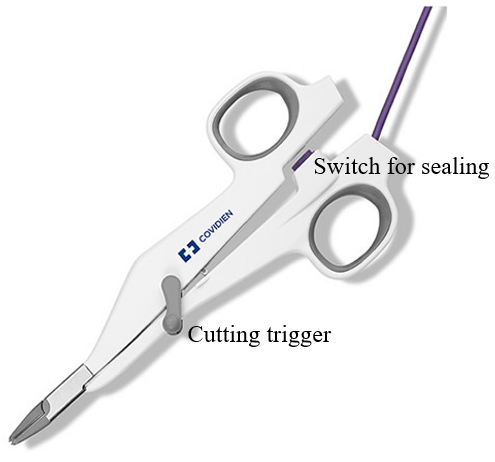
Figure 1: ‘LigaSureTM Small Jaw’ disposable vessel sealing device.
Although its usefulness as a surgical device is well-known, many hospitals in Japan currently (tend to) hesitate to use it except for extended cancer surgery because of surgical-cost-increase due to its price and disposability. Therefore, other devices which allow multiple usages can be one of the solutions, such as ‘marClampCut IQ’ (KLS Martin, Tuttlingen, Germany) [9]. Both ‘LigaSure small jaw’ and ‘marClampCut IQ’ have similar capabilities: tissue dissection, sealing and resection with a single instrument, extremely low thermal lateral spread (less than 2 mm), easy handling and reprocessing.
In this study, both devices, the disposable device ‘LigaSure small jaw’ and the reusable device ‘marClampCut IQ’ (Figure 2), were retrospectively compared and verified with the focus on (1) hemostasis, (2) surgical time and (3) medical expenses for oral cancer patients who received modified total neck dissection in our hospital and related facilities.
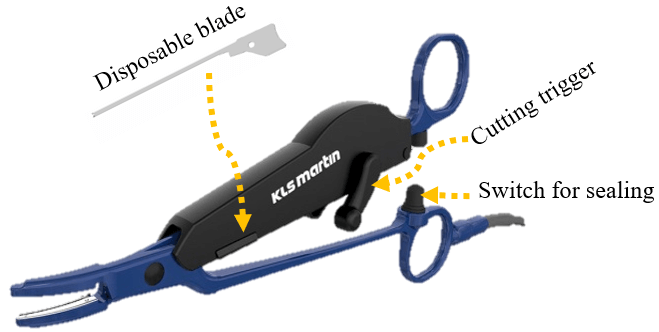
Figure 2: ‘marClampCut IQ’ reusable vessel sealing device. Only blade is discarded after each surgery and the device itself can be sterilized and reused.
Materials and Methods
All surgical procedures were carried out by the corresponding author at the department of oral and maxillofacial surgery, Tsurumi University dental hospital and general hospitals, which are related facilities of the department. Between October 2014 and April 2020, modified total neck dissections were performed with the disposable vessel sealing device, ‘LigaSure small jaw’ for 56 oral cancer patients aged from 26 y/o to 88 y/o (median = 66.0 y/o) (‘LigaSure small jaw’ group). On the other hand, the same surgical treatments were performed with the new reusable device, ‘marClampCut IQ’ between November 2018 and April 2020 for 64 oral cancer patients aged from 31 y/o to 91 y/o (median = 70.5 y/o) (‘marClampCut IQ’ group).
Both instruments were used for tissue preparation, vessel sealing, and subsequent tissue resection under standard settings with appropriate electric voltage and current, which were automatically calculated from the impedance level whenever each device would seal the organ during surgery. In addition to the usage, the blades of ‘marClampCut IQ’ were changed for each surgical treatment, and the body was properly sterilized by autoclave at 134°C (273.2°F) for 20 minutes according to ISO 17665-1.
The evaluated points were 1) patients’ age, 2) amount of intraoperative blood loss, and 3) operation time, and all the results were statistically analysed between the ‘LigaSure small jaw’ group and the ‘marClampCut IQ’ group by Mann-Whitney U-test and differences detected by univariate analyses, which were regarded as statistically significant at P < 0.05 (EZR software, Saitama Medical Center, Jichi Medical University, Saitama, Japan) [10]. The cost of each device per surgical treatment was calculated based on the prices determined by the companies.
Results
I Patients’ Ages
The medians of patients’ ages in the ‘LigaSure small jaw’ group and the ‘marClampCut IQ’ group were 66.0 y/o (26 - 88 y/o) and 75.0 y/o (31 – 91 y/o), respectively. There was no significant difference between two groups (P = 0.087) (Figure 3).
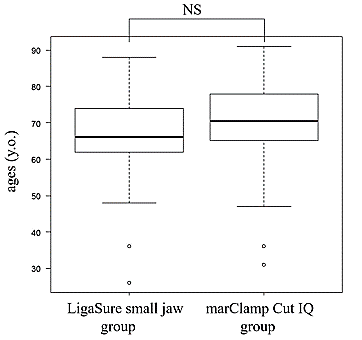
Figure 3: Comparison of “LigaSure small jaw” group and “marClampCut IQ” group with respect to patients’ ages (y/o). Median age of each group was 66 y/o. (range 26-88y/o.) and 70.5y/o. (range 31-91y/o.), respectively. There was no significant difference (Mann-Whitney U-test, P = 0.087).
NS: not significant.
II Blood Loss and Surgical Time
The median amounts of blood loss in the ‘LigaSure small jaw’ group and the ‘marClampCut IQ’ group were 30g (range: 12-56g), and 25g (range: 5-62g), respectively, and the median surgical times of modified total neck dissection (excluding time for resection of carcinoma and reconstruction) of each group were 64 minutes (range: 55-78 minutes) and 62 minutes (range: 49-76 minutes), respectively.
III Statistical Analysis
The blood loss in the ‘LigaSure small jaw’ group was significantly different from that in the ‘marClampCut IQ’ group (P = 0.006) (Figure 4). On the other hand, surgical times of the two groups did not show significant difference (P = 0.098) (Figure 5).
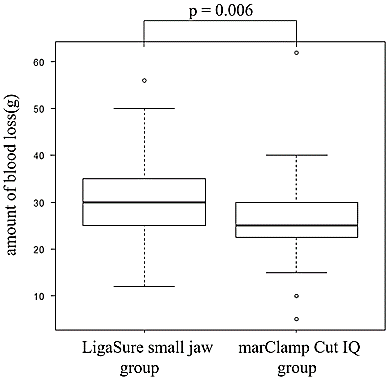
Figure 4: Comparison of ‘LigaSure small jaw’ group and ‘marClamp Cut IQ’ group with respect to amount of blood loss(g). The median amount of blood loss for each group was 30g (range 12g-56g) and 25g (range 5g-62g), respectively. There was significant difference between two groups (Mann-Whitney U-test, P = 0.006).
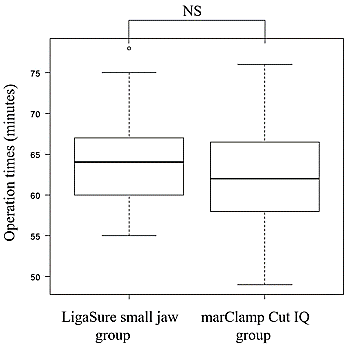
Figure 5: Comparison of ‘LigaSure small jaw’ group and ‘marClampCut IQ’ group with respect to operation times only for neck dissection (minute). Operation times of each group was 64 minutes (range: 55-78 minutes) and 62 minutes (range: 46-76 minutes), respectively. There was no significant difference in operation time between the two groups (Mann-Whitney U-test, P = 0.098).
NS: not significant.
IV Cost Savings for Operation
The prices per unit of ‘LigaSure small jaw’ and ‘marClampCut IQ’ were approximately 1,000 USD and 7,000 USD, respectively. Considering that the blade of ‘marClampCut IQ’ was disposable and its cost was approximately 100 USD, and the quality of it was guaranteed up to 50-time-usages by the manufacturer. Then, the practical cost of ‘marClampCut IQ’ for each operation amounted to 240 USD, resulting in 760 USD cost savings for each operation.
Discussion
The concept of cost-effectiveness in medical care used to be a taboo for both patients and medical institutes. However, the concept of quality of life has been focused on, and the increase of healthcare expenditure has serious implications and may possibly cause severe financial problems for patients. The importance of cost-effectiveness in medical treatment is now one of the prominent issues in the medical field [11-13]. Moreover, medical institutes have also began considering this issue to balance the increased demand for quality treatment and the financial profit from the medical industry.
On the other hand, the expenditure on healthcare in each country is quite different according to their own system [14]. Owing to the universal healthcare system, the share of the insured individual in Japan is only 0-30% (Link). However, the medical fee system has been revised once in two years, and the financial situation is highly unpredictable due to the increased cost for social welfare in a super-aging society. For example, the medical fee for total neck dissection is currently determined to be 200,800 JPY (approximately 1,900 USD) by the board of National Health Insurance, and the fee of neck dissection is included in that of primary cancer resection. Therefore, the medical fee of resection of primary cancer with or without neck dissection is exactly the same. In this financial circumstance, the concept of cost-effectiveness and reduction of medical cost should also be important for the sake of financial management of hospitals in addition to highly qualified medical service, highly skilled surgical technique, and safety in all the procedures.
Both the devices used in this research are considered suitable for comparative analysis on the basis of many previous reports from many kinds of surgical treatment, not only for craniofacial surgery but also for abdominal surgery [15, 16]. Moreover, to offer the same quality of surgical treatment and avoid bias from technical difference between surgeons, all the procedures for neck dissection were performed by one surgeon (the corresponding author).
To the best of our knowledge, there has not been any comparative study between ‘LigaSure small jaw’ and ‘marClampCut IQ’ till date. In the present study, ‘marClampCut IQ’ showed decrease in the hemostasis level and a surgical cost-cut compared to ‘LigaSure small jaw’. From this result, it is suggested that ‘marClampCut IQ’ would possibly provide the same effects for other surgical procedures. The only concern is that ‘marClampCut IQ’ requires thorough washing, followed by sterilization after surgery for prevention of infection, which may lead to more time and cost consumption. Depending on the sterilization system of institutes or countries, disposable ‘LigaSure small jaw’ may have higher potency for cost-reduction compared to ‘marClampCut IQ’. Therefore, more investigation would be highly necessary to obtain a better understanding of the choice of devices and cost-effectiveness in surgical treatment.
Conclusion
In this report, compared to the disposable device ‘LigaSure small jaw’, the reusable device ‘marClampCut IQ’ provided similar clinical efficacy for modified neck dissection, and the cost per surgical procedure was significantly reduced to the level of one-quarter.
Conflicts of Interest
None.
Ethical Approval
This clinical study was retrospectively evaluated using approved devices. Therefore, ethical approval by the Institutional Board of Tsurumi University Dental Hospital was not required.
Consent
The approval for publication was obtained from all patients.
Article Info
Article Type
Research ArticlePublication history
Received: Thu 09, Jul 2020Accepted: Fri 24, Jul 2020
Published: Wed 29, Jul 2020
Copyright
© 2023 Koji Kawaguchi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JSO.2020.04.05
Figures & Tables
NS: not significant.
NS: not significant.
References
- Prabhjyot Singh, Daniel O'Connell, Moran Langille, Peter Dziegielewski, Michael Allegretto et al. (2010) LigaSure versus conventional hemostasis in thyroid surgery: prospective randomized controlled trial. J Otolaryngol Head Neck Surg 39: 378-84. [Crossref]
- Giuseppe Colella, Amerigo Giudice, Antonio Vicidomini, Pasquale Sperlongano (2005) Usefulness of the LigaSure vessel sealing system during superficial lobectomy of the parotid gland. Arch Otolaryngol Head Neck Surg 131: 413-416. [Crossref]
- Hou Shan Yao, Qiang Wang, Wei Jun Wang, Can Ping Ruan (2009) Prospective clinical trials of thyroidectomy with LigaSure vs conventional vessel ligation: a systematic review and meta-analysis. Arch Surg 144: 1167-1174. [Crossref]
- Prakobkiat Hirunwiwatkul, Sutumma Tungkavivachagul (2013) A multicenter, randomized, controlled clinical trial of ligasure small jaw vessel sealing versus conventional technique in thyroidectomy. Eur Arch Otorhinolaryngol 270: 2109-2114. [Crossref]
- El Eraian AM, El Azeem EA, Mahamound AAH (2013) Skin sparing mastectomy made easy with the use of LigaSure Impact TM and tumescent local anesthesia towards technical standardization. Med J Cairo Univ 81: 85-95.
- Ian M Thompson 3rd, Stephen F Kappa, Todd M Morgan, Daniel A Barocas, Carl J Bischoff et al. (2014) Blood loss associated with radical cystectomy: a prospective, randomized study comparing Impact LigaSure vs. stapling device. Urol Oncol 32: 45.e11-e15. [Crossref]
- Mami Kanamoto, Satoru Imura, Yuji Morine, Tohru Utsunomiya, Hiroki Mori et al. (2015) Effective use of a vessel-sealing system for laparoscopic unroofing of liver cysts. Asian J Endosc Surg 8: 91-94. [Crossref]
- Marco Del Chiaro, John Blomberg, Ralf Segersvärd, Elena Rangelova, Christoph Ansorge et al. (2014) The use of LigaSureTM does not affect histologic margin assessment in pancreaticoduodenectomy (PD) specimens. JOP 15: 597-599. [Crossref]
- Maximilian Klar, Jörg Haberstroh, Sylvia Timme, Gernod Fritzsch, Gerald Gitsch et al. (2011) Comparison of a reusable with a disposable vessel-sealing device in a sheep model: efficacy and costs. Fertil Steril 95: 795-798. [Crossref]
- Y Kanda (2013) Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 48: 452-458. [Crossref]
- Luca Lorenzoni, Annalisa Belloni, Franco Sassi (2014) Health-care expenditure and health policy in the USA versus other high-spending OECD countries. Lancet 384: 83-92. [Crossref]
- Aleksandra Harat, Maciej Harat, Melissa Martinson (2020) A Cost-Effectiveness and Quality of Life Analysis of Different Approaches to the Management and Treatment of Localized Prostate Cancer. Front Oncol 10: 103. [Crossref]
- Satoshi Kodera, Arihiro Kiyosue, Jiro Ando, Hiroshi Akazawa, Hiroyuki Morita et al. (2017) Cost-effectiveness analysis of cardiovascular disease treatment in Japan. Int Heart J 58: 847-852. [Crossref]
- Koechlin F, Konijn P, Lorenzoni L, Schreyer P (2017) Comparing Hospitals and Health Prices and Volumes Across Countries: A New Approach. Soc Indic Res 131: 43-64.
- K L Harold, H Pollinger, B D Matthews, K W Kercher, R F Sing et al. (2003) Comparison of ultrasonic energy, bipolar thermal energy, and vascular clips for the hemostasis of small-, medium-, and large-sized arteries. Surg Endosc 17: 1228-1230. [Crossref]
- Kerem Ozturk, Isa Kaya, Goksel Turhal, Arin Ozturk, Gulce Gursan et al. (2016) A comparison of electrothermal bipolar vessel sealing system and electrocautery in selective neck dissection. Eur Arch Otorhinolaryngol 273: 3835-3838. [Crossref]