Right-Sided Bochdalek Hernia with Cecum Perforation
A B S T R A C T
Background: A Bochdalek hernia is one of the most frequently occurring congenital diaphragmatic hernias, and it occurs in 1 out of 2,500 births. Clinical cases of adults with symptomatic Bochdalek hernias are very rare. We describe a patient with an incarcerated Bochdalek hernia who underwent emergency surgery and presented with a recurrence after three years. Comparable cases in the literature were reviewed.
Case Presentation: A 56-year-old woman presented to the emergency department with acute dyspnea and pain in the epigastrium shortly after gastroscopy. A CT scan showed right sided intrathoracic herniation of the ascending colon and signs of perforation of a hollow viscus. During the operation, a suture repair of a cecal perforation as well as of a diagrammatic lesion was performed. The thorax and abdomen were lavaged and drained. The postoperative course was uneventful. After 3 years, the patient presented with colic pain in the upper abdominal quadrants. A small recurrence of the Bochdalek hernia was observed on a computed tomography scan and was managed with watchful waiting. A systematic search of comparable acute cases of Bochdalek hernias was performed.
Conclusion: An incarcerated right colon with a perforation in a Bochdalek hernia is extremely rare; only 11 comparable cases of right sided Bochdalek hernia with acute symptoms are described in the literature. Recurrent Bochdalek hernias are even rarer. As a delay in the diagnosis or a missed diagnosis can ultimately lead to death, adequate imaging is warranted when considering a recurrence of a Bochdalek hernia.
Keywords
Bochdalek hernia, intrathoracic cecum, cecum perforation, surgical repair
Background
In 1848, a Bochdalek hernia (BH) was first described [1]. With an incidence of 1 in 2500 live births, BH represents approximately 80% of all congenital diaphragmatic hernias [2]. However, the prevalence of BH in adults is only 0.17% [1, 3]. Approximately 78% of all BH are left-sided, 20% are right-sided, and 2% are bilateral [4, 5]. During the 4th week of gestation, the diaphragm begins to develop and is usually fully formed by 9 weeks of gestation [6]. BH occurs due to incomplete closure of the pleuroperitoneal membrane of the posterolateral portion of the diaphragm [7, 8]. We describe a case of an adult woman with acute abdominal and pulmonary complaints due to a BH with an incarcerated colon, which is complicated with a recurrence three years after the primary repair. Comparable cases in the literature were reviewed.
Case Presentation
A 56-year-old woman presented to the emergency department (ED) with progressive dyspnea and pain in the epigastrium and right hemithorax after an uneventful gastroscopy without biopsies for unexplained iron deficiency anemia earlier that day. The patient did not have a history of abdominal or thoracic trauma. The patient’s comorbidities included: rheumatoid arthritis without indication for anti-inflammatory drugs, hypertension, diabetes mellitus type 2 and obesity.
A physical examination at the ED revealed thoracic asymmetry, diminished breathing sounds on the right thorax by auscultation, and no signs of peritonitis. The patient had a tachycardia event, and the oxygen saturation level was 86%. The chest X-ray showed a pneumothorax and atelectasis in the right lobe. An atypical air configuration in the right lower thorax was observed (Figure 1). The patient’s respiratory function and hemodynamics were stable at that point. Therefore, the drainage of the pneumothorax was postponed, and an intravenous contrast-enhanced computed tomography (CT) of the thorax and abdomen was immediately performed, which showed a large pneumothorax with a mild shift of the mediastinum and heart to the left, pleural effusion, atelectasis, and a defect in the right diaphragm with intrathoracic herniation of the ascending colon and a small part of the transverse colon (Figure 2). The terminal ileum was thickened, and signs of inflammation were located in the right upper quadrant.
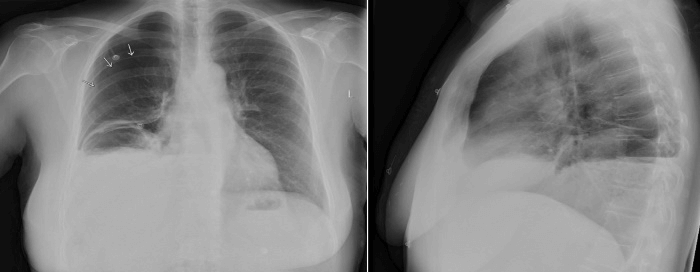
Figure 1: Chest X-ray before surgery.
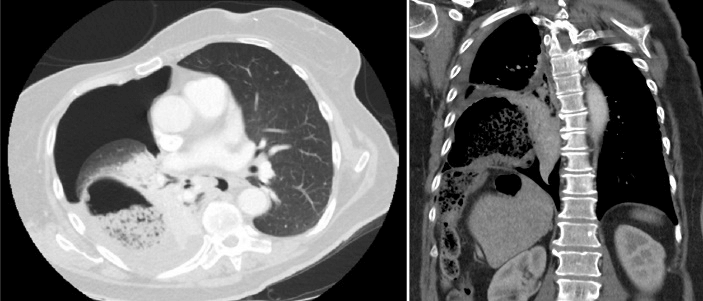
Figure 2: Axial and coronal computed tomography images before surgery. A right-sided Bochdalek hernia with herniation of the colon is shown.
Due to suspicion of an intrathoracic perforation of the herniated colon, the patient underwent an emergency laparotomy, 3.5 hours after ED admission. The period between the onset of symptoms and surgery was approximately 14 hours. Before the incision was made, 2 grams of cefazolin were administered. Surgical access was obtained through a right subcostal incision. There was a defect in the right diaphragm without a hernia sac. The herniated colon was replaced from the thorax to the abdomen. The intestines, gallbladder, and liver were inspected for vitality and lesions. A perforated cecum was observed and closed with PDS 3-0. An abdominal drain was placed below the diaphragm. The right hemithoracic cavity revealed a significant amount of pus. Therefore, lavage was performed, and a thoracic drain was placed. Primary suture repair of the diaphragmatic defect was performed with Vicryl 1 (Ethicon, Amersfoort, The Netherlands).
Postoperatively, the patient was admitted to the intensive care unit for two days. Postoperative antibiotic treatment consisted of metronidazole and ceftriaxone for five days. The chest drain was removed on the 1st postoperative day, and the abdominal drain was removed on the 2nd postoperative day. The postoperative recovery period was uneventful. Enteral feeding was started the day after surgery, and after seven days, the patient was discharged. At the six-month follow-up examination, there was no clinical or radiological evidence of hernia recurrence. The preoperative atypical abdominal pain had disappeared.
After 3 years, the patient presented with frequent pain in the upper abdomen, radiating to her back. Symptoms occurred once a week, lasted for minutes to hours, and started and ended abruptly. The patient sometimes felt the urge to move during the pain episodes. As she recognized some of the complaints, she feared the recurrence of a BH. At the physical examination, the patient had normal breathing sounds and a painful right upper quadrant of the abdomen during palpation. She had no fever.
Our differential diagnoses were symptomatic gallstones, kidney stones, adhesions after surgery or recurrence of a BH. Gallstones were excluded by transabdominal ultrasound. A chest X-ray suggested a recurrence of a BH (Figure 3). Therefore, a CT scan was performed, which confirmed a small recurrence of the BH with partial herniation of the liver (Figure 4). Because of expected adhesions of the liver against the diaphragm, after the surgery performed 3 years earlier, the change in herniation of other organs was considered to be minimal. The risk of complications and chance of recurrence after a reoperation were weighted against watchful waiting and discussed with the patient. Furthermore, an opinion from surgeons not related to the case was obtained. They concluded that if the patient chooses surgery or complaints worsen, the preferred approach is a laparoscopic procedure with adhesiolysis, full mobilization of the liver, and mesh stabilization of the diaphragm. However, this kind of surgery was not preferred when complaints would be bearable. Therefore, watchful waiting was chosen. A month later, the symptoms had reduced.
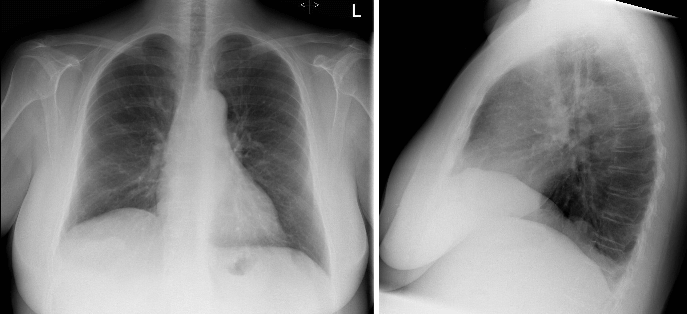
Figure 3: Chest X-ray 3 years after operation. Slight elevation of the right hemidiaphragm with a round structure at the base of the right lung is shown, suggesting a possible small recurrence of a Bochdalek hernia.
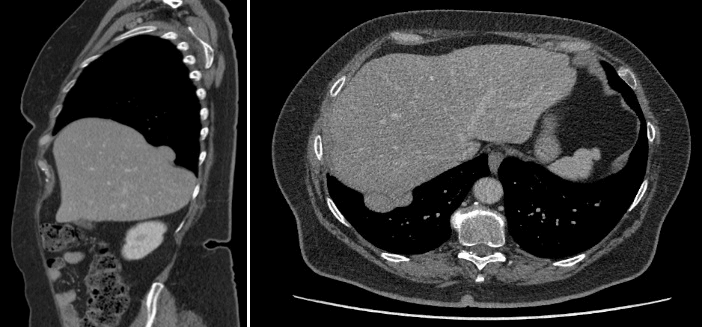
Figure 4: CT scan 3 years after operation, showing small recurrence of a Bochdalek hernia with partial liver parenchyma herniation.
Discussion and Conclusion
Symptomatic BH in adults are extremely rare, and the clinical presentation varies from vague complaints to acute pain in the abdomen [1]. Consequently, complicated BH are rarely suspected, and the diagnosis is often delayed [9, 10]. This affects prognosis; a mortality rate of 2.7-12% has been reported in previous studies [1, 11, 12]. Due to the rarity of these cases, little is known about the follow-up period, long-term complications or the chance of recurrence. To achieve a good outcome in cases of incarcerated BH, early diagnosis is important.
Table 1: Available literature of right-sided Bochdalek hernias in adults with acute symptoms.
|
First author (Reference) |
Gender |
Age (years) |
Symptoms |
Diagnostic imaging |
Herniated organ |
Operative approach |
Length of hospitalization (days) |
Follow-up (months) |
Test at follow-up |
Condition at follow-up |
|
Costa Almeida [15] |
Female |
49 |
Cough, sputum and worsening dyspnea |
Chest X-ray CT scan
|
Cecum, ileo-cecal appendix, right colon and transverse colon |
Laparotomy |
13 |
24 |
Unknown
|
Asymptomatic, no recurrence
|
|
Deb [8] |
Male1 |
54 |
Nausea, epigastric pain |
CT scan
|
Stomach, liver, bowel, omentum |
Laparotomy |
Unknown
|
12
|
Chest X-ray |
Asymptomatic, no recurrence |
|
Frisoni [18] |
Female |
39 |
Dyspnea, abdominal and right shoulder pain |
CT scan MRI |
Right colon |
Thoracoscopy |
Unknown
|
1 and 6 months
|
CT at 1 month
|
Asymptomatic, no recurrence |
|
Granier [16] |
Female |
54 |
Acute dyspnea |
Chest X-ray CT scan
|
Terminal ileum, up to the middle part of the right colon |
Explorative laparotomy
|
Died during admission |
- |
- |
- |
|
Ohtsuka [11] |
Female |
89 |
Dyspnea, abdominal pain and vomiting |
Chest X-ray CT scan
|
Terminal ileum to transverse colon
|
Laparotomy
|
78 |
24
|
Unknown |
Asymptomatic, no recurrence
|
|
Salustio [17] |
Female |
50 |
Generalized abdominal pain, distension, vomiting and constipation |
Chest X-ray CT scan |
Ileum
|
Explorative laparotomy
|
21 |
Unknown
|
Unknown
|
No complications were identified during follow-up
|
|
Shenoy [19] |
Male |
60 |
Dyspnea, periumbilical abdominal pain, vomiting |
Chest X-ray US-abdomen CT scan
|
Small bowel
|
Laparotomy
|
Unknown
|
Unknown
|
Unknown
|
Unknown
|
|
Wenzel-Smith [20] |
Female |
40 |
Severe abdominal pain, nausea, vomiting, constipation, dyspnea |
Chest X-ray
|
Small bowel
|
Laparotomy
|
12
|
1
|
Unknown
|
Superficial wound sepsis, no hernia recurrence
|
|
Debergh [13] |
Female |
38 |
Severe abdominal pain for hours, nausea and vomiting |
US-abdomen (due to pregnancy)
|
Small bowel
|
Explorative laparoscopy
|
8
|
12
|
Unknown
|
Free from recurrence
|
|
Pindoria [14] |
Female2 |
21 |
Intermittent sharp right upper quadrant pain and increasing dyspnea |
Chest X-ray MRI (due to pregnancy) |
Small bowel, liver, right kidney, renal ureter and vessels
|
Laparoscopic
|
7
|
Unknown
|
CT scan |
Unknown
|
|
Kanazawa [21] |
Female |
63 |
Dyspnea and abdominal pain |
Chest X-ray CT scan |
Ascending and transverse colon and right kidney |
Laparotomy and right thoracotomy |
Unknown
|
Unknown
|
Unknown
|
Unknown
|
1 Positive history of Bochdalek hernia.
2 Patient had undergone a right-sided hernia repair at 12 days after birth.
A literature search of patients older than 18 years who underwent emergency surgical repair due to acute symptoms of a right-sided BH revealed 11 case reports in PubMed (Figure 5). The diagnosis, treatment, outcome, and follow-up results were reviewed. The results are shown in (Table 1). Out of the 11 cases, 9 patients were females. Two patients were pregnant, and both were in the second trimester [13, 14]. Most patients showed acute dyspnea, abdominal pain or signs of gastrointestinal obstruction at presentation to the ED. However, cases without abdominal pain were also described [8, 11, 15]. Various imaging techniques were used for the diagnosis. In multiple cases, a chest X-ray initially raised suspicion for a BH, followed by a CT scan to confirm the diagnosis of the BH. Of the 11 patients, 8 underwent an acute laparotomy. Three patients were treated laparoscopically or thoracoscopically. Two patients had perforations of a hollow viscus: 1 had a perforated cecum, and 1 had a perforated ileum [16, 17]. The diaphragmatic defect was repaired with a mesh in 3 patients and was repaired with non-absorbable sutures in 8 patients. One patient died during admission due to septic shock from necrotizing fasciitis.
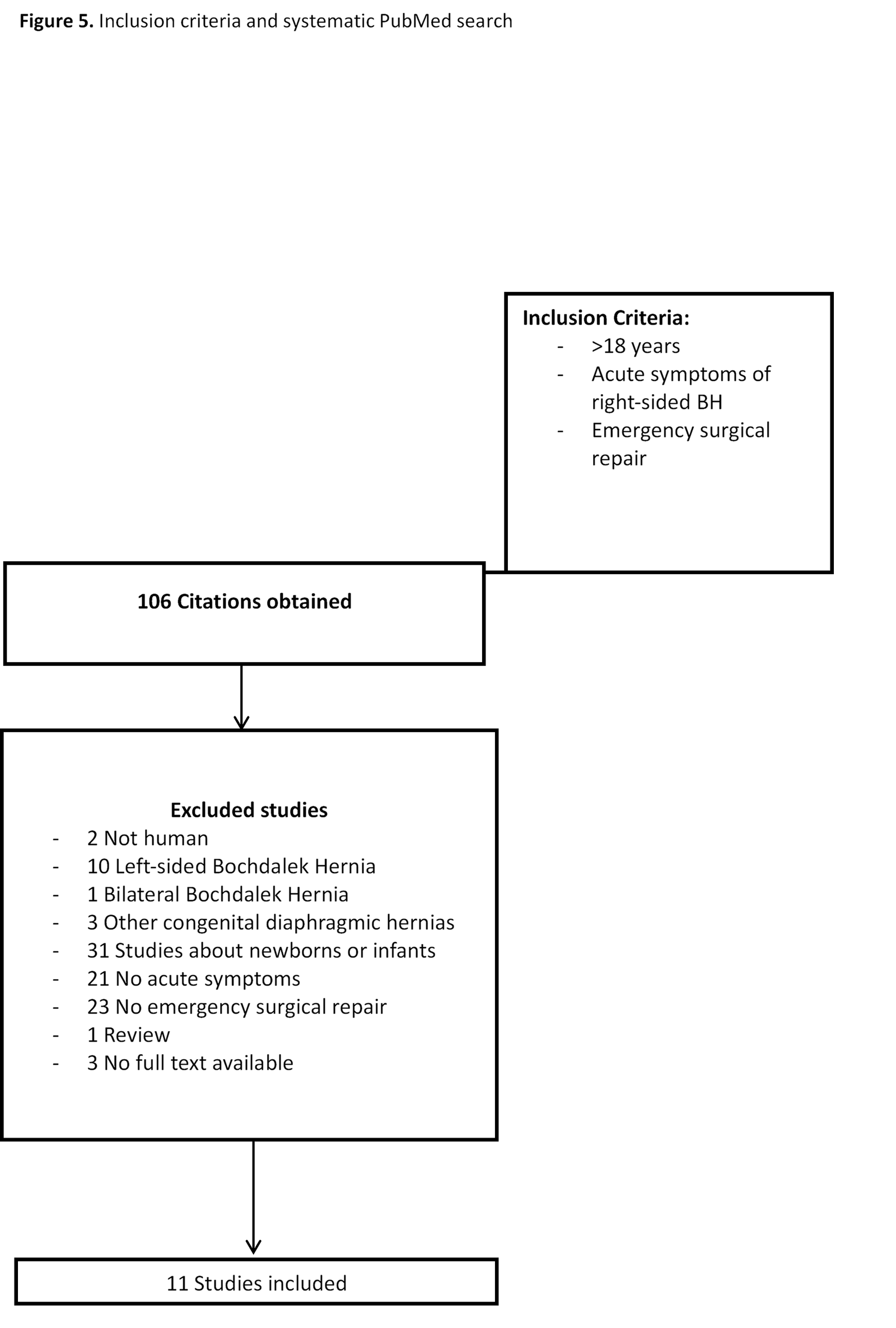
Figure 5: Inclusion criteria and systematic PubMed search.
At the follow-up (1 to 24 months), 5 patients were asymptomatic and showed no signs of recurrence. In 3 cases, the conclusions at the follow-up were based on imaging. The only study describing the recurrence rate is that conducted by Machado et al. They described a recurrence rate of 1,6% (3 of 184 adults) in a group of patients in whom the majority underwent elective operations. Symptoms or diagnostic modalities to detect recurrence were not described [1].
The patient in our study developed a recurrence of the BH without acute symptoms. However, in one of the 11 included studies in our literature search, Pindoria et al. described a pregnant woman who underwent right-sided hernia repair in early childhood (at the age of 12 days), developed a recurrence in her second trimester of pregnancy, and underwent an acute laparoscopic repair [14]. Based on these data, it is difficult to make a recommendation on the follow-up schedule or intervention. In our case, we had 2 intervention options. The first was watchful waiting, and the second was an elective surgery with adhesiolysis, mobilization of the liver and repair of the hernia with mesh. The first treatment option is almost without complications. However, the second option is associated with a high risk of surgical complications. We chose for watchful waiting because the complaints were bearable and even had reduced after one month. There is a chance of recurrence of complaints and acute circumstances, although this chance is considered low. Given that the risk of a delayed or missed diagnosis is high and management plans are unclear, we advocate adequate diagnostic imaging, such as a CT or MRI scan, in cases of dyspnea or (a)typical abdominal pain, when the recurrence of a BH is considered.
The clinical manifestation of a BH in adults is atypical, and the incidence is very low. In acute cases, rapid diagnosis and surgical intervention are required. This case report described a patient with atypical abdominal pain due to a recurrence of a BH 3 years after surgical repair of an incarcerated hernia with cecal perforation. As a delay in the diagnosis or a missed diagnosis can ultimately lead to death, adequate imaging is warranted when considering the recurrence of a BH.
Ethical Approval
The name of the ethics committee examined the study: Prof. Dr. P.N.R. Dekhuijzen, Chairman, Research Ethics Committee, Radboud University Nijmegen Medical Centre. The committee’s reference number (file number CMO): 2019-5566.
Consent
Consent for publication was obtained from the patient presented in our case report.
Availability of Data and Materials
Not applicable.
Competing Interests
None.
Funding
None.
Author Contributions
TN: drafted the work and substantively revised it, designed the work, interpreted the data, and revised the manuscript; EJ: drafted the work and substantively revised it, interpreted the data, and revised the manuscript; DF: designed the work, drafted the work, and interpreted the data. MH: interpreted the data and designed the work; OB: drafted the work and substantively revised it and interpreted the data; HG: have drafted the work and substantively revised it, designed the work, interpreted the data, and revised the manuscript; All authors read and approved the final manuscript. All authors agreed both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Acknowledgements
Not applicable.
Abbreviations
BH: Bochdalek hernia
ED: Emergency Department
CT: Computed tomography
MRI: Magnetic resonance imaging
Article Info
Article Type
Case ReportPublication history
Received: Wed 04, Mar 2020Accepted: Sat 21, Mar 2020
Published: Wed 25, Mar 2020
Copyright
© 2023 Tina Natroshvili. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.03.04
Figures & Tables
Table 1: Available literature of right-sided Bochdalek hernias in adults with acute symptoms.
|
First author (Reference) |
Gender |
Age (years) |
Symptoms |
Diagnostic imaging |
Herniated organ |
Operative approach |
Length of hospitalization (days) |
Follow-up (months) |
Test at follow-up |
Condition at follow-up |
|
Costa Almeida [15] |
Female |
49 |
Cough, sputum and worsening dyspnea |
Chest X-ray CT scan
|
Cecum, ileo-cecal appendix, right colon and transverse colon |
Laparotomy |
13 |
24 |
Unknown
|
Asymptomatic, no recurrence
|
|
Deb [8] |
Male1 |
54 |
Nausea, epigastric pain |
CT scan
|
Stomach, liver, bowel, omentum |
Laparotomy |
Unknown
|
12
|
Chest X-ray |
Asymptomatic, no recurrence |
|
Frisoni [18] |
Female |
39 |
Dyspnea, abdominal and right shoulder pain |
CT scan MRI |
Right colon |
Thoracoscopy |
Unknown
|
1 and 6 months
|
CT at 1 month
|
Asymptomatic, no recurrence |
|
Granier [16] |
Female |
54 |
Acute dyspnea |
Chest X-ray CT scan
|
Terminal ileum, up to the middle part of the right colon |
Explorative laparotomy
|
Died during admission |
- |
- |
- |
|
Ohtsuka [11] |
Female |
89 |
Dyspnea, abdominal pain and vomiting |
Chest X-ray CT scan
|
Terminal ileum to transverse colon
|
Laparotomy
|
78 |
24
|
Unknown |
Asymptomatic, no recurrence
|
|
Salustio [17] |
Female |
50 |
Generalized abdominal pain, distension, vomiting and constipation |
Chest X-ray CT scan |
Ileum
|
Explorative laparotomy
|
21 |
Unknown
|
Unknown
|
No complications were identified during follow-up
|
|
Shenoy [19] |
Male |
60 |
Dyspnea, periumbilical abdominal pain, vomiting |
Chest X-ray US-abdomen CT scan
|
Small bowel
|
Laparotomy
|
Unknown
|
Unknown
|
Unknown
|
Unknown
|
|
Wenzel-Smith [20] |
Female |
40 |
Severe abdominal pain, nausea, vomiting, constipation, dyspnea |
Chest X-ray
|
Small bowel
|
Laparotomy
|
12
|
1
|
Unknown
|
Superficial wound sepsis, no hernia recurrence
|
|
Debergh [13] |
Female |
38 |
Severe abdominal pain for hours, nausea and vomiting |
US-abdomen (due to pregnancy)
|
Small bowel
|
Explorative laparoscopy
|
8
|
12
|
Unknown
|
Free from recurrence
|
|
Pindoria [14] |
Female2 |
21 |
Intermittent sharp right upper quadrant pain and increasing dyspnea |
Chest X-ray MRI (due to pregnancy) |
Small bowel, liver, right kidney, renal ureter and vessels
|
Laparoscopic
|
7
|
Unknown
|
CT scan |
Unknown
|
|
Kanazawa [21] |
Female |
63 |
Dyspnea and abdominal pain |
Chest X-ray CT scan |
Ascending and transverse colon and right kidney |
Laparotomy and right thoracotomy |
Unknown
|
Unknown
|
Unknown
|
Unknown
|
1 Positive history of Bochdalek hernia.
2 Patient had undergone a right-sided hernia repair at 12 days after birth.
References
- Machado NO (2016) Laparoscopic Repair of Bochdalek Diaphragmatic Hernia in Adults. N Am J Med Sci 8: 65-74. [Crossref]
- Stege G, Fenton A, Jaffray B (2003) Nihilism in the 1990s: the true mortality of congenital diaphragmatic hernia. Pediatrics 112: 532-535. [Crossref]
- Hunter LM, Mozer AB, Anciano CJ, Oliver AL, Iannettoni MD et al. (2019) Robotic-Assisted Thoracoscopic Repair of Right-Sided Bochdalek Hernia in Adults: A Two-Case Series. Innovations (Phila) 14: 69-74. [Crossref]
- Brown SR, Horton JD, Trivette E, Hofmann LJ, Johnson JM (2011) Bochdalek hernia in the adult: demographics, presentation, and surgical management. Hernia 15: 23-30. [Crossref]
- Mohan G, Kalyanaraman S, Ramakrishnan S, Theodore S (2018) Concomitant diaphragmatic hernia repair with coronary artery bypass grafting surgery. Ann Card Anaesth 21: 304-306. [Crossref]
- GC S (2009) Larsen’s Human Embryology. 4th ed. Philadelphia ed. Churchill Livingstone.
- Ayane GN, Walsh M, Shifa J, Khutsafalo K (2017) Right congenital diaphragmatic hernia associated with abnormality of the liver in adult. Pan Afr Med J 28: 70. [Crossref]
- Deb SJ (2011) Massive right-sided Bochdalek hernia with two unusual findings: a case report. J Med Case Rep 5: 519. [Crossref]
- Rout S, Foo FJ, Hayden JD, Guthrie A, Smith AM (2007) Right-sided Bochdalek hernia obstructing in an adult: case report and review of the literature. Hernia 11: 359-362. [Crossref]
- Kohli N, Mitreski G, Yap CH, Leong M (2016) Massive symptomatic right-sided Bochdalek hernia in an adult man. BMJ Case Rep 2016: bcr2016217432. [Crossref]
- Ohtsuka Y, Suzuki TH (2017) Right-sided Bochdalek hernia in an elderly patient: a case review of adult Bochdalek hernias from 1982 to 2015 in Japan. Acute Med Surg 4: 209-212. [Crossref]
- Kumar A, Maheshwari V, Ramakrishnan T, Sahu S (2009) Caecal perforation with faecal peritonitis - unusual presentation of Bochdalek hernia in an adult: a case report and review of literature. World J Emerg Surg 4: 16. [Crossref]
- Debergh I, Fierens K (2014) Laparoscopic repair of a Bochdalek hernia with incarcerated bowel during pregnancy: report of a case. Surg Today 44: 753-756. [Crossref]
- Pindoria N, Makanjuola J, Botha A, Nair R, Thurairaja R (2018) "What Goes Up Must Come Down": Laparoscopic Retrieval of a Migrated Intrathoracic Kidney and Repair of Recurrent Symptomatic Diaphragmatic Hernia. J Endourol Case Rep 4: 129-132. [Crossref]
- Costa Almeida CE, Reis LS, Almeida CM (2013) Adult right-sided Bochdalek hernia with ileo-cecal appendix: Almeida-Reis hernia. Int J Surg Case Rep 4: 778-781. [Crossref]
- Granier V, Coche E, Hantson P, Thoma M (2010) Intrathoracic caecal perforation presenting as dyspnea. Case Rep Med 2010: 296730. [Crossref]
- Salustio R, Nabais C, Paredes B, Sousa FV, Porto E et al. (2014) Association of intestinal malrotation and Bochdalek hernia in an adult: a case report. BMC Res Notes 7: 296. [Crossref]
- Frisoni R, Germain A, Ayav A, Brunaud L, Bresler L (2014) Thoracoscopic treatment of a right Bochdalek hernia in an adult (with video). J Visc Surg 151: 239. [Crossref]
- Shenoy KR, Johri G (2013) Congenital right bochdalek hernia presenting as emergency in old age: a case report. Indian J Surg 75: 255-256. [Crossref]
- Wenzel Smith G (2013) Posterolateral diaphragmatic hernia with small-bowel incarceration in an adult. S Afr J Surg 51: 73-74. [Crossref]
- Kanazawa A, Yoshioka Y, Inoi O, Murase J, Kinoshita H (2002) Acute respiratory failure caused by an incarcerated right-sided adult bochdalek hernia: report of a case. Surg Today 32: 812-815. [Crossref]