Robotic-Assisted Endoscopic Resection of an Ectopic Ureter Draining into the Urethra in a Female Patient
A B S T R A C T
Ectopic ureters are rare in the population. We report a case of an ectopic ureter draining into the urethra in a young female. The ectopic ureter was resected in robotic assisted surgery. The urinary continence was normal at 2 years follow-up.
Keywords
Ureter, robotic surgery, continence
Introduction
The estimated prevalence of duplex kidneys ranges between 0.3% and 6% of the population, with a female preponderance [1]. An ectopic ureter is defined as any ureter with its orifice draining at the bladder neck or beyond. Incidence varies between 1:2000 and 1:4000 [2]. An ectopic ureter increases the risk for urinary tract infections (UTI) and has been found in 8% of patients presenting with recurrent UTI. Ureteral duplication is commonly diagnosed in childhood. In adults, the diagnostic pathway may be more complex. This is the first description of an ectopic ureter that drained into urethra being managed successfully via a robot-assisted approach.
Case Presentation
The patient is a 25-year-old female with a childhood history of frequent urinary tract infections that disappeared spontaneously. Seven years ago, she suffered an episode of pyelonephritis followed by several urinary tract infections in spite of antibiotic prophylaxis. An abdominal CT scan revealed a duplex kidney with two complete ureters and a large, dilated upper kidney pelvis without function in the upper pole. The distal part of the ectopic ureter was dilated up to 12 mm. The lower pole ureter followed the usual course into the bladder, with the ureter orifice at the trigone. The patient had frequency but no bladder-related pain, incontinence or dyspareunia. Her voiding diary indicated that she had 12 micturitions per day with a maximal volume of 600 ml. The patient’s gynecological status revealed no abnormalities. In preoperative endoscopic inspection and MRI imaging of the bladder and urethra, the ectopic ureter drained into the urethra at the bladder neck just above sphincter (Figure 1).
The patient underwent surgery, starting with a cystourethroscopy. The draining of the ectopic ureter was seen at 4 to 5 o’clock (Figure 2). A guidewire was placed into the lower pole ureter. A robot-assisted resection of the ectopic ureter was then performed. Port placement was similar to that of prostatectomy [3]. The left sigmoid colon was mobilized, and ureters were identified. The ectopic ureter was ligated with Haemolock® and cut, followed by mobilization distally along the ureter below the tuba uterina and uterine artery up to the bladder neck. The bladder was mobilized anteriorly. The ectopic ureter (Figure 3) was cut at the urethral wall and closed with two 4-0 PDS sutures. An indwelling catheter was in place for 7 days.
The patient was discharged 3 days postoperatively. At 4 days after surgery, she was admitted to emergency due to high fever and left flank pain. A CT scan revealed a dilatation in the upper part of the ectopic ureter and upper pole pelvis. At 5 days postoperative an open upper pole resection of the kidney was performed through lumbar incision including removal of the rest of the ectopic ureter with favorable results. Broad-spectrum antibiotics were administrated for 7 days with favorable results. Blood culture was positive for Streptococcus pneumoniae. The postoperative period was uneventful. The pathologist’s report showed minor inflammatory reactions in the removed ureter. At four weeks follow-up, the patient had normal continence but still some pain in the lumbar area. She had symptoms and suspicion of UTI 6 and 8 months postoperatively. However, urine culture revealed no bacterial infection. She was treated twice with pivmecillinam antibiotics three days with favorable results. At 2 years follow-up, she had no symptoms and continence was normal.
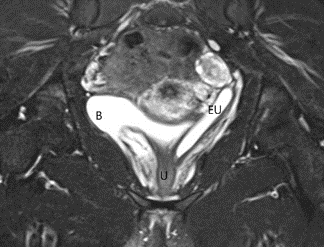
Figure 1: MRI scan showing the dilated ectopic ureter on the left. B=bladder, EU=ectopic ureter, U=urethra.
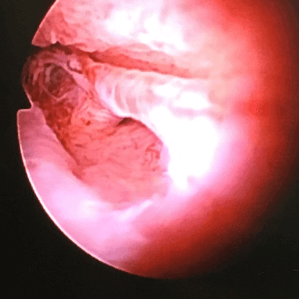
Figure 2: Endoscopic view into the urethra at the level of the external urinary sphincter showing the orifice of the ectopic ureter into the ureter.
Discussion
Ureteral duplication and ectopic upper pole ureters are quite rare and there is no consensus regarding the treatment of these patients. Usually they are diagnosed and treated in childhood, and therefore symptoms and diagnoses are rare in adults. The presence of an ectopic ureter is associated with vesicoureteral reflux, obstruction and infections. In this case, infections were frequent, and obstruction or reflux caused dilatation of the ectopic ureter. The patient ended up in a second emergency surgery to resect the upper pole pelvis and the remaining ectopic ureter at postoperative day 5. The imaging studies did not show function in the upper pole, but there was still minor urine output causing dilatation and infection of the remaining ureter, which could have been identified at an earlier stage in scintigraphy. Upper pole resection of the kidney with removal of the ectopic ureter remains the best option for treating such an anomaly.
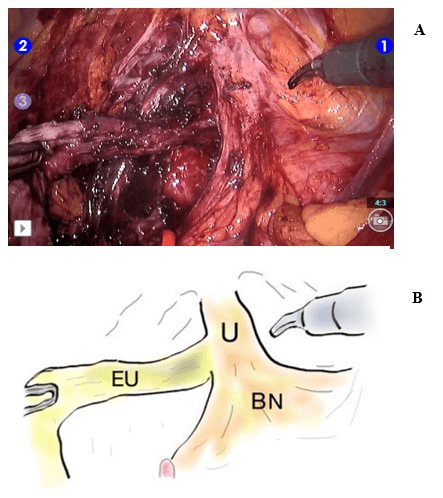
Figure 3: (A) View into the pelvis during robotic surgery. The instrument holding the ectopic ureter on the left demonstrates the course of the ectopic ureter. (B) Figure showing EU=ectopic ureter, BN=bladder neck and U=urethra
Conclusion
This case highlights that anatomical variations may cause urinary tract infections and thorough examination should not be neglected. Functional imaging should be included in the assessment of the remaining upper pole stage. Robot-assisted laparoscopic removal of the ectopic ureter is one feasible treatment option with good cosmesis and a functional outcome.
Acknowledgement
None.
Statement of Ethics
The study complies with the guidelines for human studies according to WMA Declaration of Helsinki. Patient has given her consent to publish details and photos of the case.
Conflicts of interest
None.
Funding
None.
Author Contributions
All authors have made substantial contribution to the manuscrpit. Robotic surgery was performed by A Petas and kidney resection by N Hendolin and J Huttunen.
Article Info
Article Type
Case ReportPublication history
Received: Mon 30, Dec 2019Accepted: Wed 15, Jan 2020
Published: Mon 27, Jan 2020
Copyright
© 2023 Anssi Petas. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.GSCR.2019.01.05
Figures & Tables
References
- Raja J, Mohareb AM, Bilori B (2016) Recurrent urinary tract infections in an adult with a duplicated renal collecting system. Radiol Case Rep 11: 328-331. [Crossref]
- Albers P, Foster RS, Bihrle R, Adams MC, Keating MA (1995) Ectopic ureters and ureteroceles in adults. Urology 45: 870-874. [Crossref]
- Pick DL, Lee DI, Skarecky DW, Ahlering TE (2004) Anatomic guide for port placement for daVinci robotic radical prostatectomy. J Endourol 18: 572-575. [Crossref]