Size Specific Dose Estimate in Abdominal Computed Tomography by AAPM TG Report-204 and AAPM TG Report-220
A B S T R A C T
Purpose: The AAPM Task Group (TG) reports 204 and 220 presented methods for evaluation of patient dose by announcing the SSDE. The TG reports provide the Size Specific Conversion factors that can be multiplied to CTDIvol to calculate the patient dose in terms of SSDE constructed from Deff (AAPM TG-204) and Dw (AAPM TG-220). Our study presents a comparison of the two TG reports on SSDE for the routine Abdominal Computed Tomography.
Materials and Methods: The scan lengths of abdomen were measured from computed tomography (CT) topographic images and cross-section at the mid-slice of the abdomen were measured from tomographic images of 61 adults who had undergone abdominal CT using the GE Advance Workstation (AWS) software. The Deff and Dw was computed according to TG- 204 and TG-220 reports, respectively. Further, we performed the correlation analysis between Deff and BMI, Dw and BMI and SSDE and BMI for both the TG- reports. The Student’s paired t-test was performed to compare the two of SSDE calculation methods.
Results: The results confirm that the mean value of SSDE is 13.04 (𝑚𝐺𝑦) and 13.60 (𝑚𝐺𝑦) for AAPM TG-220 and AAPM TG-204, respectively. And a good positive correlation was observed between Deff and BMI, Dw and BMI with r = 0.67 and r = 0.68 respectively. Also, the weak correlation was observed between SSDE and BMI for both the TG - reports. The Student’s paired t-test shows that the two means of SSDE calculation methods are significantly different (𝑝< 0.01) in abdominal computed tomography.
Conclusion: We confirm the AAPM TG reports 204/220 using clinical data for SSDE calculation that the mean SSDE values computed from Deff and Dw in abdomenal computed tomography are significantly different and we conclude that the SSDE calculated by Dw method gives a more accurate evaluation of SSDE for the patients undergoing abdominal computed tomography scan then the SSDE calculated by Deff method.
Keywords
Size specific dose estimate, effective diameter, water equivalent diameter, radiation dose
Introduction
Computed tomography (CT) is one amongst the major important imaging modality in medical science. Since the development of CT in the 1970s, it has transformed the medical science and diagnostic decision-making, nevertheless the manoeuvre of such powerful skill demands that the radiation professional to judge the essentiality of patient safety in addition to image quality and diagnostic usefulness. CT imaging offers widespread information to diagnose, plan treatment and evaluate many diseases in patients [1]. The radiation dose to patients and professionals from CT is at all times a common concern among the healthcare professionals [2, 3]. This is mainly because of the increasing number of CT examinations and high dose from CT compared to other imaging modalities [3-5]. Usually entrance or skin dose has been used for conventional radiography [6]. For CT, since x-rays are directed on the patient from 360° view, the surface or skin dose does not present an idea about the maximum absorbed dose [7, 8]. It is always a challenge for radiation professionals to establish adequate image quality with minimum radiation exposure to the patient in agreement with ALARA (As Low As Reasonably Achievable) principle [9]. As a consequence, we rely on metrics for dose estimation such as Computed Tomography Dose Index Volume (CTDIvol, mGy) and Dose Length Product (DLP, mGym). In order to demonstrate the radiation doses, the International Electrochemical Commission (IEC) requires all scan manufacturers to display radiation output with descriptors such as CTDIvol and DLP before and after the examination in the form of dose page or image [6-10]. One of the major flaws of CTDIvol is that it does not characterize genuine patient absorbed doses, as it does not take into account the heterogeneous attenuation and size of the individual patients [11-13].
The American Association of Physicists in Medicine (AAPM) Task Group (TG) Report 204 came up with the concept of a size-specific dose estimate (SSDE) [14]. The SSDE is a patient size-corrected estimate of radiation dose received by the patient, which uses a replacement for patient dose to scale the scanner reported CTDIvol.The TG report 204 details the use of multiple size surrogates to normalize CTDIvol values to SSDE including: anterior-posterior (AP) dimensions, Lateral (LAT) dimensions, AP + LAT, circumference, and effective diameter (AP × LAT)1/2. The size surrogates of AAPM TG Report 204, however, are based only on patient geometry and do not think about the differential attenuations of diverse tissue types within the human body. This inadequacy was addressed in the AAPM TG Report 220 in detail, and proposed the term water-equivalent diameter (Dw), and its applications in finding dose received by the patient [15]. The central intent of the TG Report 220 was to develop a concrete metric for automatically estimating patient size that would account for patient differential attenuation and allow routine calculation of SSDE for all patients, with least user involvement. The Dw represents the diameter of a cylinder of water that contains the same total x-ray attenuation as that contained within the patient’s axial cross section and depends on both the cross-sectional area of the patient and the attenuation of the contained tissues. The purpose of our study is to compute the Size Specific Dose Estimate Comparison in Abdominal CT imaging and to present the comparison of AAPM TG Report 204 and AAPM TG Report 220.
Material and Methods
I Patients
This prospective study was approved by our Institutional Ethics Committee (Ref. No.: IECJNMC/612, Feb-2022). The committee waived off the written consent because the patients were already scheduled for a CT and were not subjected to an additional unnecessary scan. The subjects included are the sixty-one adult patients undergoing “routine” abdominal CT examination between 01.03.2022 and 30.04.2022 for different clinical indications. The exclusion criteria were as follows: 1) patients with poor cooperation during the examination, 2) patients who were re-scanned owing to operational errors or patient’s reasons, 3) poor quality of imaging and, 4) Patients who had foreign or metal fixator bodies on the body surface.
II Imaging Protocol
All patients underwent a CT scan of the abdomen with a standard protocol using the following parameters: Patients were placed in a spine position with head first. The scanning range was from the lung apex to the pubic symphysis and the CT examination was performed with a Wipro GE Healthcare Revolution EVO 3.68B MID BJG, 128 slice CT unit installed in our department as per the standard imaging Protocol. The pre-set parameters were as follows: tube voltage (kVp: 80 – 120), quality reference (mAs: 100) detector collimation (128 × 0.6 mm), acquisition matrix (512 × 512), field-of-view [(314 × 314 mm), slice acquisition thickness (5 mm) and inter-slice spacing (1 mm).
III Computation of Size Specific Dose Estimate (SSDE)
i AAPM TG Report-204
In order to estimate SSDE, conversion factors from the look up tables of the AAPM TG report- 204 for the 32 cm phantom size (same as recorded phantom size on our cases dose page report) were multiplied by CTDIvol, since tables do not include diameters with decimals, all diameters with decimals were rounded to the nearest whole number values. In addition, SSDE values greater than 0.5 mGy were reported as rounded off whole number values and for 0.5 mGy only one decimal number was reported. The effective diameter (Deff) of abdominal CT was measured by mid-slice of the scanning region using digital callipers by calculating the anterior-posterior (AP) and lateral dimensions on each selected axial image of the CT abdomen and the fallowing equation was used by the AAPM TG report-204 to calculate the (Deff):
\[D_{eff} = (AP × LAT)^{1/2}........(1)\]
The SSDE mGy was computed by the specific formula for a specific patient size:
\[SSDE = f_{size}^{32x} × CTDI_{vol}........(2)\]
Where \[f_{size}^{32x}\] is the conversion factor based on CTDIvol specified in the AAPM TG report-204 on SSDE. The CTDIvol is the average absorbed dose inside a scan volume in relation to a standard 32 cm CT phantom diameter. The conversion factor values were derived from dimensions of the patient noted from GE Advance Workstation (AWS) software.
ii AAPM TG Report-220
The sole use of water-equivalent diameter (Dw), takes into account the differential tissue attenuation in addition to patient geometric dimensions for calculation of SSDE is recommended. The SSDE is CTDIvol with multiplicative conversion factors (fsize) which depends on Dw as described in the TG report-220. The Dw was determined by axial CT images. The CTDIvol and DLP are displayed on the monitor of GE Advance Workstation (AWS) software based on 32 cm Phantom in all the examinations. The SSDE and Dw was also computed according to the AAPM report-220 from the following equations:
\[SSDE = f_{size}^{32x} × CTDI_{vol}^{32}........(3)\] \[f_{size}^{32x} = a × e^{-b × D_{W}}........(4)\] \[D_{W}=2\sqrt{(\frac{ROI_{mean}}{1000}+1)}×\sqrt{\frac{A_{ROI}}{\pi}}........(5)\]
Where ROImean is the mean CT number in the Region of interest (ROI), HU; AROI is the total area of the ROI (cm2); ROImean and AROI were automatically calculated by team play according to the axial CT images. \[f_{size}^{32x}\] are the conversion factors. Where a= 0.4378 and b= 0.043 are the normalized dose coefficients for the 32 cm PMMA CTDIvol data as function of Dw. The normalized coefficients are the results of the three independent research groups, the curve fit shows excellent agreement across all data points, with a correlation coefficient of 0.967.
III Body Mass Index (BMI) Measurement
All the patients had weight and height measurements performed and their BMI was calculated immediately prior to the CT imaging scan using a dedicated calibrated device (Indosurgicals: weight and height measuring machine). The BMI data was used to sub divide the patient groups, where under-weight referred to BMI < 18.5 kgm-2, normal weight referred to 18.5 ≤ BMI ≤ 24.9 kgm-2, overweight referred to 25 ≤ BMI ≤ 29.9 kgm-2, and obese referred to BMI ≥ 30 kgm-2.
IV Statistical Analysis
Origin 6.0 [v6.1052 (B232) Origin Lab Corporation, Northampton, MA 01060 USA] software was used for all the data analysis. The student’s paired t-test was performed to compare the two SSDE methods provided by the two TG reports (i.e., AAPM TG-report-204 and AAPM TG report-220). The p-value less than 0.01 (p < 0.01) was considered statistically significant. Mean and standard deviation were computed for patient age, CTDIvol, Deff, Dw and SSDE. In order to evaluate the dependence of Deff, Dw and SSDE on BMI, the correlation analysis was performed between Deff and BMI, Dw and BMI, SSDE and BMI.
Results
The study population (n= 61) comprised of 28 men and 33 women with an age of 45.39±17.91 (mean±Std. dev) years, ranging from 20 to 86 years. The overall BMI was 20.8±4.43 (mean±Std. dev) kgm-2, ranging from 13.30 to 36.26 kgm-2. The 17 patients had BMI less than 18.50 kgm-2 (underweight), 5 patients had BMI between 25.0 to 29.90 kgm-2 (overweight), 3 patients had BMI greater then 30.0 kgm-2 (obese) and 36 patients had BMI between 18.50 and 24.90 kgm-2. The mean CTDIvol(mGy), DLP(mGym2), and SSDE(mGy) calculated from the AAPM TG report - 204 and AAPM TG report - 220 are listed in the (Table 1). The average value was Deff(cm) 23.84±3.36 cm, ranging from 17 to 32 cm and the mean of Dw(cm) was 24.93 ± 3.70 cm, ranging from 18.0 to 33.0 cm as presented in the (Table 1).
Table 1: Statistical data of patient
demography, CTDIvol, DAP, Deff, Dw
|
|
Mean |
Std. dev. |
Std. error |
Min. |
Max. |
|
Age(years) |
45.39 |
±17.91 |
±2.29 |
20 |
86 |
|
Deff
(cm) |
23.84 |
±3.36 |
±0.43 |
17 |
32 |
|
CTDIvol(mGy) |
8.88 |
±1.99 |
±0.25 |
4.39 |
14.10 |
|
DLP(mGy) |
477.93 |
±262.94 |
±33.67 |
186.38 |
1466.20 |
|
Dw
(cm) |
24.93 |
±3.70 |
±0.47 |
18 |
33 |
|
BMI (kGm-2) |
20.82 |
±4.43 |
±0.57 |
13.30 |
36.26 |
|
SSDE(mGy)TG - 204 |
13.60 |
±2.72 |
±0.35 |
7.31 |
23.07 |
|
SSDE(mGy)TG
- 220 |
13.04 |
±2.54 |
±0.32 |
7.04 |
22.23 |
The correlation analysis was performed in order to find the dependence of the effective diameter Deff(cm) on BMI, water equivalent diameter Dw(cm) on BMI and Size Specific Dose Estimate (SSDE, mGy) computed by the two TG reports with BMI. A good positive correlation was found between Deff(cm) and BMI (r= 0.67) and Dw(cm) and BMI (r= 0.68) as revealed in the (Figures 1 & 2). The SSDE computed by the TG - 204 and TG- 220 were weakly correlated with the BMI with (r= 0.57) and (r= 0.54) respectively as presented in the (Figures 3 & 4). The two SSDE calculation methods were compared statistically by student’s paired t-test at 99% level of significance (p <0.01). The student’s paired t- test presents a comparison of two SSDE measurement methods in the (Table 2) and the two means were found significantly different at 99% level of significance with p= 0.0001.

Figure 1: Correlation analysis between effective (Deff) and Body Mass index (BMI).
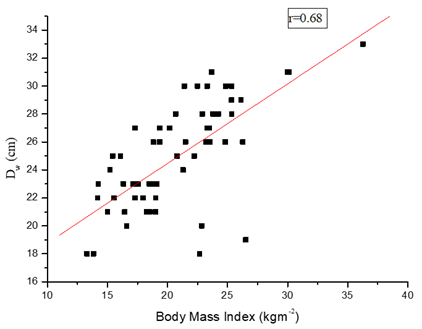
Figure 2: Correlation analysis between effective (Dw) and Body Mass index (BMI).

Figure 3: Correlation analysis between effective SSDE (TG - 204) and Body Mass index (BMI).

Figure 4: Correlation analysis between effective SSDE (TG - 220) and Body Mass index (BMI).
Table 2: Student’s paired
|
Method |
Number of Patients |
Mean SSDE (mSv) |
Variance of SSDE (mSv) |
t - value |
p
- value |
|
AAPM TG - 204 |
61 |
13.60 |
7.41 |
7.85 |
|
|
AAPM TG - 220 |
61 |
13.04 |
6.47 |
Discussion
AAPM Task Group-204 and 220 introduced the concept of using anterior-posterior, lateral, effective diameter (Deff) and water equivalent diameter (Dw) of the patient to calculate the Size Specific Dose Estimate (SSDE). In AAPMTG -204, SSDE is a dose parameter that takes into consideration correction based on the size of the patient from the linear dimensions measured from the patient images. The SSDE is an estimate of a mean dose to the center of the scan volume for the patient having similar attenuation characteristics as of a given patient; it is now a direct measurement of dose to a specific patient [16]. The conversion factors used to calculate SSDE from CTDIvol report in the AAPM TG report - 204 were derived from the experimental and Monte Carlo data normalized to patient size in terms of water or tissue equivalent material. The AAMPM Task Group - 220 confirmed that the Deff was 4.3% to 21.5% greater than Dw in thorax because the Deff considers only the geometry but not the differential attenuation that could lead to an overestimate of SSDE [17]. This limitation was addressed in the AAPM Task Group - 220 and developed the technique by using the attenuation of x-rays through the body as measured by CT scanner, to calculate patient water equivalent diameter Dw, the diameter of a cylindrical volume of water with equivalent mean attenuation. This study was about radiation dose in adult abdominal CT exam, the SSDE calculation was decided by both Deff and Dw. The CTDIvol, DLP, Deff and Dw of abdominal CT examinations increased as the patient size increased in the present study and there was a good positive correlation for both Deff and Dw with BMI with r= 0.67 and r= 0.68 respectively. This was expected because both Deff and Dw are directly related to the patient dimensions. A weak positive correlation was also observed for SSDE and BMI for both Deff and Dw calculations with r= 0.57 and r= 0.54 respectively. The mean and variance of the SSDE calculated from Dw were found less than the SSDE calculated from Deff and the Student’s paired t- test shows that two means are significantly different at 99% level of significance with p< 0.01. The Deff considered only the patient geometry but not the attenuation that could lead to an over estimate of the patient size and to the under estimation or over estimation of SSDE. The Dw calculation of SSDE considers the influence of the scanning parameters, patient size, and differential x-ray attenuation on the radiation dose, which gives more realistic estimate of radiation dose for patients undergoing CT examination and is less likely to under estimate patient radiation dose compared with the Deff method as explained by the student’s paired t- test statistics.
Conclusion
In the present study the two AAPM Task Group reports (i.e., AAPM TG -204 and AAPMTG- 220) for the calculation of size specific dose estimate were compared statistically by Student’s paired t- test at 99% level of significance (p < 0.01). We infer from the (Table 2) the two means were significantly different with p= 0.0001 and we conclude that the SSDE calculation by Dw (i.e., AAPM TG -220) method considers the influence of scanning parameters, patient size and x-ray attenuation on the radiation dose, gives a more realistic estimate of radiation dose for patients undergoing abdominal CT examination then the SSDE calculation by Deff (i.e., AAPM TG-204) method which takes into account the patient geometry only.
Article Info
Article Type
Research ArticlePublication history
Received: Sat 08, Apr 2023Accepted: Tue 09, May 2023
Published: Thu 07, Sep 2023
Copyright
© 2023 Mudasir Ashraf Shah. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.RDI.2023.01.01
Figures & Tables
Table 1: Statistical data of patient
demography, CTDIvol, DAP, Deff, Dw
|
|
Mean |
Std. dev. |
Std. error |
Min. |
Max. |
|
Age(years) |
45.39 |
±17.91 |
±2.29 |
20 |
86 |
|
Deff
(cm) |
23.84 |
±3.36 |
±0.43 |
17 |
32 |
|
CTDIvol(mGy) |
8.88 |
±1.99 |
±0.25 |
4.39 |
14.10 |
|
DLP(mGy) |
477.93 |
±262.94 |
±33.67 |
186.38 |
1466.20 |
|
Dw
(cm) |
24.93 |
±3.70 |
±0.47 |
18 |
33 |
|
BMI (kGm-2) |
20.82 |
±4.43 |
±0.57 |
13.30 |
36.26 |
|
SSDE(mGy)TG - 204 |
13.60 |
±2.72 |
±0.35 |
7.31 |
23.07 |
|
SSDE(mGy)TG
- 220 |
13.04 |
±2.54 |
±0.32 |
7.04 |
22.23 |
Table 2: Student’s paired
|
Method |
Number of Patients |
Mean SSDE (mSv) |
Variance of SSDE (mSv) |
t - value |
p
- value |
|
AAPM TG - 204 |
61 |
13.60 |
7.41 |
7.85 |
|
|
AAPM TG - 220 |
61 |
13.04 |
6.47 |
References
1.
International Commission
on Radiological Protection (ICRP) (2000) Managing
Patient Dose in Computed Tomography. publication 87 3.
2.
Brenner DJ, Elliston CD,
Hall EJ, Berdon WE (2001) Estimated
risks of radiation induced fatal cancer from paediatric CT. AJR Am J
Roentgenol 176: 289–296. [Crossref]
3.
Kalender WA (2014) Dose in x-ray computed tomography. Phys
Med Biol 59: R129–R150. [Crossref]
4.
IAEA (2011) Status of computed tomography: dosimetry for
wide cone beam scanners. Human
Health Report, Vienna: International Atomic Energy Agency.
5.
Bauhs JA, Vrieze TJ,
Primak AN, Bruesewitz MR, McCollough CH (2008) CT dosimetry: comparison of measurement techniques and devices. Radiographics
28: 245–253. [Crossref]
6.
George J, Eatough JP,
Mountford PJ, Koller CJ, Oxtoby J (2004) Patient
dose optimization in plain radiography based on standard exposure factors.
Br J Radiol 77: 858-863. [Crossref]
7.
Pooley RA, McKinney JM,
Miller DA (2001) The AAPM/RSNA physics
tutorial for residents: digital fluoroscopy. Radiographics 21:
521-534. [Crossref]
8.
Report of AAPM Task
Group 23: CT Dosimetry. (2014) The
Measurement, Reporting and Management of Radiation Dose in CT.
9.
Lee CH, Goo JM, Ye HJ,
Ye SJ, Park CM et al. (2008) Radiation
dose modulation techniques in the multidetector CT era: from basics to
practice. Radiographics. 28: 1451. [Crossref]
10. International Electrochemical
Commission (IEC) Evaluation and
routine testing in medical imaging departments Part 26: Constancy tests
imaging performance of computed tomography X-ray equipment. IEC 61223-2-6
ed2.0.
11. Huda W, Scalzetti EM, Roskopf M
(2000) Effective doses to patients
undergoing thoracic computed tomography examinations. Med Phys
27: 838-844. [Crossref]
12. McCollough CH, Leng S, Yu L, Cody
DD, Boone JM et al. (2011) CT dose
index and patient dose: they are not the same thing. Radiology
259: 311-316. [Crossref]
13. Li X, Samei E, Williams CH, Segars
WP, Tward DJ et al. (2012) Effects of
protocol and obesity on dose conversion factors in adult body CT. Med
Phys 39: 6550-6571. [Crossref]
14. Report of AAPM Task Group 204 (2012)
Size-Specific Dose Estimates (SSDE) in Paediatric and Adult Body CT
Examinations.
15. Report of AAPM Task Group 220 (2014)
Use of Water Equivalent Diameter for calculating patient Size and Size Specific
Dose Estimate (SSDE) in CT.
16. Christer JA, Braun NM, Jacobsen MC, Carter RE, Kofler JM et al. (2012) Size specific dose estimate for adult patients at CT of the torso. Radiology 265: 841-847. [Crossref]
17. Hu X, Gou J, Lin W, Zou C, Li W (2021) Size-specific dose estimates of adult, chest computed tomography examinations: Comparison of Chinese and updated 2017 American College of Radiology diagnostic reference levels based on the waterequivalent diameter. PLoS ONE 16: e0257294. [Crossref]