Synchronous Bilateral Breast Cancer: Implications for Adjuvant Radiation
A B S T R A C T
We present the case of a 55-year old postmenopausal female with bilateral early stage clinically node negative breast cancer who was treated with bilateral lumpectomy with axillary lymph node dissection revealing N1a nodal disease in her right breast with extra-nodal extension and micrometastatic disease in her left breast. Given the controversy in management for low nodal burden for macroscopic and microscopic nodal disease, we review the key trials in regional nodal management that have included patients with low nodal burden to explain our reasoning for treatment decisions. Our patient was treated with both hypofractionation and conventional treatment. She is an excellent teaching case to demonstrate how much of an impact the decision regarding fractionation can have on long term breast cosmesis and toxicity.
Keywords
Bilateral breast cancer, hypofractionation, conventional fractionation, cosmesis
Introduction
Synchronous bilateral breast cancer poses a unique challenge in that a treatment must be devised for each cancer while taking into account the added technical complexity of bilateral treatment and the additional considerations of two treatment courses for a single patient. Bilateral breast cancer is uncommon with an incidence of 1-3% with rates of synchronous bilateral breast cancer of 2.1% and often occur in younger patients with early stage disease [1-3]. Despite prior controversies regarding effects of bilateral breast cancer on prognosis, more recent papers suggest there are no differences in mortality and often both sides have similar biology [4-7]. Bilateral mastectomy previously was the standard treatment, but rates of bilateral breast conservation have steadily increased over time along with the complexity of radiation treatment planning [6, 8].
Despite rapidly increasing choices regarding dose, fractionation, and axillary management there are no guides to assist decision making for bilateral breast treatment. We present the case of a postmenopausal female with bilateral clinically node negative breast cancer who was treated with bilateral lumpectomy with axillary lymph node micrometastatic disease in her left breast and macrometastatic disease on the right breast. She was treated with whole breast irradiation with hypofractionation (HF) to the left breast and conventional fractionation (CF) with regional nodal irradiation on the breast and axilla with macrometastatic disease. This patient demonstrates the differential toxicity of different radiation fields and fractionations and serves as an important example of how the decisions regarding adjuvant radiation of each breast cancer must be made interdependently in synchronous bilateral breast cancer.
Case
A 55-year old post-menopausal female presented with radiographically detected bilateral clinically node negative breast cancer. She underwent right (6:00) and left (2:00) partial mastectomies, sentinel lymph node (LN) biopsies with intraoperative frozen sections which were positive bilaterally and triggered completion bilateral axillary LN dissections (ALND). Surgical pathology on the right breast revealed moderately differentiated 0.8 cm invasive ductal carcinoma (IDC) with 2/9 positive LN with extra-nodal extension (ENE), ER/PR 99% HER2 negative, Ki-67 5% (pT1bN1a). On the left side, pathology revealed moderately differentiated 0.85 cm IDC with 1/10 LN with micrometastatic disease measuring 0.019 mm, ER 98% PR 2% HER2 negative, Ki-67 5% (pT1bN1mi). She had similar volumes of tissue removed from both breasts and axilla with a total volume of 130 cc on the left and 127 cc on the right breast. She received adjuvant chemotherapy with CMF for 8 cycles.
Discussion
Regarding adjuvant radiation, the recommendation was made for whole breast irradiation (WBI) and regional nodal irradiation (RNI) on the right and WBI alone on the left. The recommendation for RNI on the right was because of her macrometastatic disease in 2 LN, particularly in the context of her younger age and presence of ENE, especially in light of trials such as the MA-20 and EORTC 22922 trials which showed a small but statistically significant benefit with RNI on 10 year disease free survival [9, 10]. In the context of micrometastatic disease and a complete ALND on the left side, the decision was made to proceed with WBI alone given her low risk of regional recurrence on that side as demonstrated by prior studies with rates of <1% [11-14]. Given the inclusion of the nodes, conventional fractionation (CF) was used on the right (5000 cGy in 25 fractions). Of note, there are ongoing trials exploring hypofractionated RNI, but the patient was off trial and thus recommended for conventional fractionation [15, 16]. Given that only WBI was recommended on the left, she was treated with a hypofractionated (HF) regimen (4005 cGy in 15 fractions). A sequential 1000 cGy boost was delivered to both the right and left lumpectomy cavities. Figure 1 depicts images taken prior to RT which reveals excellent baseline cosmesis and symmetry on the day of her simulation. The patient had small breast separation (<25 cm) which allowed for excellent dose homogeneity in her treatment plans PTV with dose ranges of 95-107% for the left hypofractionated breast and dose ranges of 93-106% for the right conventionally fractionated breast.
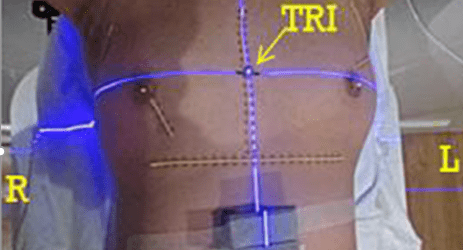
Figure 1: Images from her simulation from the day of her CT simulation.

Figure 2: Images from her follow-up appointment 1 year after completion of RT in the supine at 45⁰ (left) and upright (right). There is marked retraction and atrophy in the right breast which received conventional fractionation.
With regard to acute toxicity, the patient developed grade 1 dermatitis in the left breast, grade 2 dermatitis in the right breast requiring xeroform dressing to the inframammary fold, and grade 1 fatigue. In terms of late toxicity, the patient was seen for follow-up 1 year after completion of RT and was noticed to have asymmetry in her breast appearance with increased fibrosis and retraction of the conventionally fractionated right breast as compared to the hypofractionated left breast. Figure 2 shows images of her during her follow-up appointment while partially supine at a 45o angle (left) and sitting upright (right).
Both her acute and late toxicity was significantly decreased on the left side which received hypofractionated treatment. In multiple seminal randomized clinical trials comparing hypofractionation and conventional fractionation, the two fractionation regimens have proven to be equivalent with regard to cancer outcomes [17, 18]. These trials have reported that hypofractionation has decreased or equivalent rates of breast shrinkage, telangiectasia, and breast edema as compared to conventional fractionation. A more recent trial from MDACC randomized 287 patients with DCIS or early stage breast cancer to CF WBI or HF WBI with a tumor bed boost. This trial demonstrated a 34% decrease in grade 2 or higher acute toxicities with HF compared to CF, including fatigue, pruritis, breast pain, dermatitis, and hyperpigmentation [19]. At 3 years, adverse patient-reported cosmesis decreased from 13.6% (n=15) with CF to 8.2% (n=8) with HF (p=0.002), thus confirming non-inferiority with HF [20]. Patients with large breast size had 18.6% decreased adverse cosmetic outcome with HF-WBI.
Our patient is unique in that she served as her own control and demonstrated improved acute and late toxicity with hypofractionation. Although her tumors were located in different quadrants, she had similar volumes of tissue removed from each breast and axilla, small breast separation, and excellent dose homogeneity in her plan which eliminates other potential explanations for the difference in her cosmesis. Her case perhaps argues for the same fractionation to be used in bilateral breast cases for long-term symmetry. Though each cancer is indeed independent and may require different treatment courses, these diseases are of course occurring at the same time in the same person and thus individual treatment plans should perhaps be modified to be more similar with regard to fractionation. Whether that fractionation needs to be conventional fractionation or hypofractionation, even when targeting the regional nodes, is an area of active study.
Conflicts of Interest
No conflicts to disclose.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgement
None.
Clinical Practice Points
- Management of synchronous bilateral breast cancer is challenging, especially in the setting of increasing use of bilateral breast conservation.
- Whole breast hypofractionation and conventional fractionation have equivalent cancer outcomes, but hypofractionation has significantly reduced acute and late toxicites.
- We present a case of a woman with bilateral early stage breast cancer and excellent postoperative cosmesis who received conventional fractionation (CF) and hypofractionated treatment who has markedly increased breast shrinkage and asymmetry from CF.
- The cosmetic effects of fractionation should be thoroughly discussed especially in patients who value cosmesis, especially as more data regarding hypofractionated regional nodal irradiation emerges.
Article Info
Article Type
Research ArticlePublication history
Received: Wed 25, Sep 2019Accepted: Mon 14, Oct 2019
Published: Thu 24, Oct 2019
Copyright
© 2023 Naamit K. Gerber. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.GCCR.2019.01.04
Figures & Tables
References
- Chaudary MA, Millis RR, Hoskins EO, Halder M, Bulbrook RD et al. (1984) Bilateral primary breast cancer: a prospective study of disease incidence. Br J Surg 71: 711-714. [Crossref]
- Kheirelseid EA, Jumustafa H, Miller N, Curran C, Sweeney K et al. (2011) Bilateral breast cancer: analysis of incidence, outcome, survival and disease characteristics. Breast Cancer Res Treat 126: 131-140. [Crossref]
- Jobsen JJ, van der Palen J, Ong F, Meerwaldt JH (2003) Synchronous, bilateral breast cancer: prognostic value and incidence. Breast 12: 83-88. [Crossref]
- Mejdahl MK, Wohlfahrt J, Holm M, Balslev E, Knoop AS et al. (2019) Breast cancer mortality in synchronous bilateral breast cancer patients. Br J Cancer 120: 761-767. [Crossref]
- Schmid SM, Pfefferkorn C, Myrick ME, Viehl CT, Obermann E et al. (2011) Prognosis of early-stage synchronous bilateral invasive breast cancer. Eur J Surg Oncol 37: 623-628. [Crossref]
- Padmanabhan N, Subramanyan A, Radhakrishna S (2015) Synchronous Bilateral Breast Cancers. J Clin Diagn Res 9: XC05-XC08. [Crossref]
- Roder D, de Silva P, Zorbas H, Kollias J, Malycha P et al. (2012) Survival from synchronous bilateral breast cancer: the experience of surgeons participating in the breast audit of the Society of Breast Surgeons of Australia and New Zealand. Asian Pac J Cancer Prev 13: 1413-1418. [Crossref]
- O'Brien JA, Ho A, Wright GP, Stempel M, Patil S et al. (2015) Breast-Conserving Surgery in Bilateral Breast Cancer. Ann Surg Oncol 22: 3389-3396. [Crossref]
- Whelan TJ, Olivotto IA, Parulekar WR, Ackerman I, Chua BH et al. (2015) Regional Nodal Irradiation in Early-Stage Breast Cancer. N Engl J Med 373: 307-316. [Crossref]
- Poortmans PM, Collette S, Kirkove C (2015) Internal Mammary and Medial Supraclavicular Irradiation in Breast Cancer. N Engl J Med 373: 317-327.
- Giuliano AE, Hunt KK, Ballman KV, Beitsch PD, Whitworth PW et al. (2011) Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. JAMA 305: 569-575. [Crossref]
- Galimberti V, Cole BF, Zurrida S, Viale G, Luini A et al. (2013) Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases (IBCSG 23-01): a phase 3 randomised controlled trial. Lancet Oncol 14: 297-305. [Crossref]
- Sola M, Alberro JA, Fraile M, Santesteban P, Ramos M et al. (2013) Complete axillary lymph node dissection versus clinical follow-up in breast cancer patients with sentinel node micrometastasis: final results from the multicenter clinical trial AATRM 048/13/2000. Ann Surg Oncol 20: 120-127. [Crossref]
- Jagsi R, Chadha M, Moni J, Ballman K, Laurie F et al. (2014) Radiation field design in the ACOSOG Z0011 (Alliance) Trial. J Clin Oncol 32: 3600-3606. [Crossref]
- Khan AJ, Poppe MM, Goyal S, Kokeny KE, Kearney T et al. (2017) Hypofractionated Postmastectomy Radiation Therapy Is Safe and Effective: First Results from a Prospective Phase II Trial. J Clin Oncol 35: 2037-2043. [Crossref]
- Wang SL, Fang H, Song YW, Wang WH, Hu C et al. (2019) Hypofractionated versus conventional fractionated postmastectomy radiotherapy for patients with high-risk breast cancer: a randomised, non-inferiority, open-label, phase 3 trial. Lancet Oncol 20: 352-360. [Crossref]
- Haviland JS, Owen JR, Dewar JA, Agrawal RK, Barrett J et al. (2013) The UK Standardisation of Breast Radiotherapy (START) trials of radiotherapy hypofractionation for treatment of early breast cancer: 10-year follow-up results of two randomised controlled trials. Lancet Oncol 14: 1086-1094. [Crossref]
- Whelan TJ, Pignol JP, Levine MN, Julian JA, MacKenzie R et al. (2010) Long-term results of hypofractionated radiation therapy for breast cancer. N Engl J Med 362: 513-520. [Crossref]
- Shaitelman SF, Schlembach PJ, Arzu I, Ballo M, Bloom ES et al. (2015) Acute and Short-term Toxic Effects of Conventionally Fractionated vs Hypofractionated Whole-Breast Irradiation: A Randomized Clinical Trial. JAMA Oncol 1: 931-941. [Crossref]
- Shaitelman SF, Lei X, Thompson A, Schlembach P, Bloom ES et al. (2018) Three-Year Outcomes with Hypofractionated Versus Conventionally Fractionated Whole-Breast Irradiation: Results of a Randomized, Noninferiority Clinical Trial. J Clin Oncol 31: JCO1800317. [Crossref]