The ADeViD Study: Alzheimer’s Dementia and Vitamin D Study
A B S T R A C T
Introduction: Aging is associated with a large increase in the prevalence of hypovitaminosis D. 25-Hydroxyvitamin D, 25(OH)D, is the best indicator for vitamin D status. Its possible role in the pathogenesis of Alzheimer’s disease (AD), the leading cause of dementia in the elderly, is particularly important. The aim of the present study was to examine the association between 25-hydroxyvitamin D (25(OH)D) and cognitive functions in a group of Italian elderly patients affected with AD.
Methods: We studied the relationship between 25(OH)D and cognitive functions assessed by MMSE (Mini Mental State Examination) in 150 consecutive elderly patients (F 76 %, age 78,66+ 6,05 years old) attending our Geriatric ambulatory for cognitive disorders with diagnosis of AD.
Results: In our sample hypovitaminosis D was present in 100% of the screened patients; 111 patients (74%) had 25(OH)D serum levels inferior to 20 ng/ml; 39 (26%) patients had serum levels included between 20 and 30 ng/ml. After adjustment for age, gender, systolic blood pressure, education, cardiovascular diseases and antihypertensive treatment, a significant relationship was observed between 25(OH)D and cognitive status. MMSE appeared significantly higher in subjects with 25(OH)D serum levels ≥ 20 ng/ml than in those with 25(OH)D < 20 ng/ml (18,42+4,33 vs 12,22+4,44; p=0,000).
Conclusion: Our results showed a relationship between 25(OH)D and cognitive impairment in patients with AD, suggesting that 25(OH)D could be involved in the onset of dementia.
Keywords
Hypovitaminosis D, elderly, Alzheimer’s disease
Introduction
Alzheimer’s disease (AD) is caracterized by a progressive decline of cognitive performance with a detrimental impact on social activies [1-3]. A restricted ultraviolet ligh exposure, low vitamin D intake and a decreased skin synthesis capacity may be related to the development of vitamin D deficiency in ageing polpulation. Hypovitaminosis D is commonly observed in elderly popolation. Its possible role in the pathogenesis of Alzheimer’s Disease is particularly important, as AD remains a pubblic health concern with no current efficient treatment.Vitamin D is a neurosteroid hormone which crosses the blood-brain barrier and binds to vitamin receptors (VDR) present in neurons and glial cells of the central nervous system including the hippocampus, the hypothalamis, the cortex and the subcortex [4-6]. 1-25 dihydroxyvitamin D, that is the active form of vitamin D, regulates the intra-neuronal calcium homeostasis via the regulation of voltage-dependent calcium channels, thus preventing necrosis and has also showen neuroprotective properties against glutamate toxicity through antioxidant effects, thus preventing apoptosis [7].
Moreover, since both 25-hydroxylase and 1α-hydroxylase are present in the central nervous system, it is plausible that local production of active vitamin D (1,25-dihydroxyvitamin D) is important for normal cognitive function [8, 9]. The aim of the present study was to examine the association between 25-hydroxyvitamin D (25(OH)D) and cognitive functions in a group of Italian elderly patients with AD.
Methods
This was a retrospective study, performed on 150 patients, attending our Geriatric Outpatient Clinics for cognitive disorders with diagnosis of AD. The inclusion criteria were: age 65 years old or older. Cognitive functions were assessed by MMSE (Mini Mental State Examination), functional dependence by scores on the ADL (Activities of Daily Living) and the IADL (Instrumental Activities of Daily Living). Blood samples were taken in a fasting state 25 (OH) D may fluctuate seasonally, it was only determined in blood samples collected between January and Juen. Information on education level, smoking status, precence of chronic disease was collected using questionnaires.
Statistical Analyses
Population characteristics are reported as mean ± standard deviation (SD) or percentages. All analyses were adjusted for age, sex, BMI, education, smoking and alcohol consumption. All analyses were performed using the Statistical Package for the Social Sciences software program version 18.0 for Windows (SPSS Inc, Chicago, IL).
Results
General characteristics of the study population are presented in (Table 1). The mean ± SD 25 (OH)D level of the total population was 12,27 ±7,46 ng/ml, in our sample hypovitaminosis D was present in 100% of the screened patients and ranges below 20 mg/dl were observed in 74% of the partecipant. Mean MMSE of the population was 13,83±5,18. Our data, demonstrate a positive relationship between circulating 25 (OH)D concentration and the MMSE test scores in AD (r=0,571, p=0,000, Figure 1). After dividing people according to 25(OH)D serum levels, (≥ or < 20 ng/ml), MMSE appeared significantly higher in subjects with 25(OH)D serum levels ≥ 20 ng/ml than in those inferior to 20 ng/ml (18,42+4,33 vs 12,22+4,44; p=0,000, Figure 2). After bivariate analysis, we created multiple linear regression models, including the selected variables, in order to assess MMSE change predictors (vitamin D, education, systolic blood pressure, mean blood pressure and pulse pressure).
Table 1: Characteristics of the sample studied.
|
No. |
150 |
|
No. with 25 (OH) D< 20ng/ml, |
111 (74%) |
|
Age, years |
78,71+6,05 |
|
Sex, M % |
24% |
|
Education ≤5 years, % |
84,5% |
|
MMSE |
13,8+5,18 |
|
ADL |
3,96+1,22 |
|
IADL |
2,61+1,69 |
|
Smoking,% |
5% |
|
Cardiovacular Diseases, % |
20,1% |
|
25 (OH) D ng/ml |
12,26+7,64 |
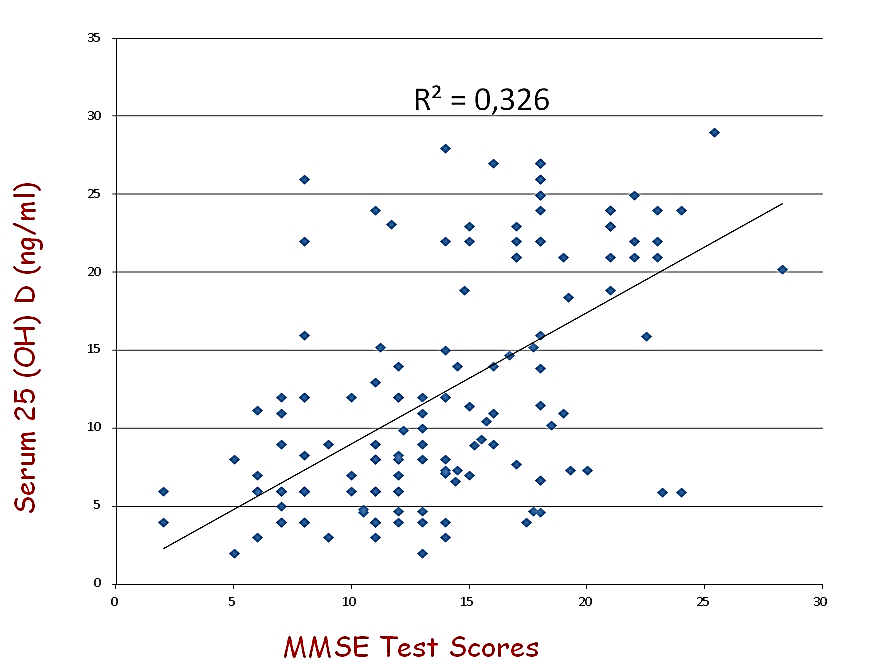
Figures 1: Relationship between MMSE Test scores and circulationg 25 (OH) D serum levels.
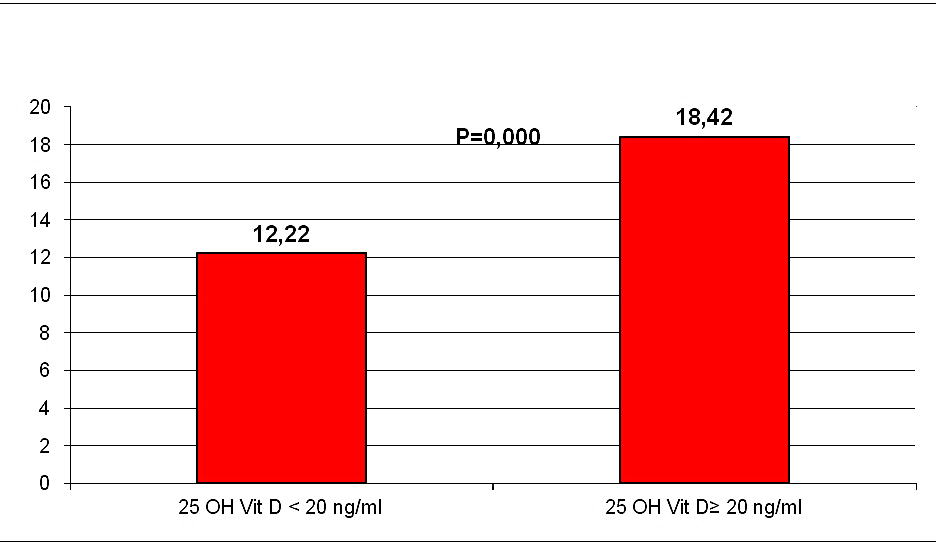
Figures 2: MMSE Test scores, after dividing people according to 25(OH) D serum levels.
In the model studied, vitamin D was the main predictor for MMSE changes (β=0.455, p<0.000). Therefore, the positive, significant correlation between 25 (OH) D concentration and MMSE score suggests the possibility that vitamin D may play a specific role in cognitive function in older adults. Measurement of circulating 25 (OH)D concentration is recognized as the best functional measure of vitamin D status [10]. Though the correct definition of vitamin D deficiency remains at present controversial, it is increasingly accepted that a serum 25 (OH)D concentration below 30 ng/ml is suboptimal [11]. Using this definition, all patient in this study had vitamin D deficiency. However, low vitamin D status has previously been reported in patient with AD [12, 13].
Discussion
A beneficial effect of vitamin D for cognition potentially could be mediated through a number of mecchanisms. It has been proposed that vitamin D may reduce the accumulation of Aβ42 peptide with an increase in the number of macrophages and polymorphonuclear leukocytes by VDR-dependent immunoregulation, specifically the phagocytosis and clearance of amyloid β peptide by macrophages [14-16]. Vitamin D-enhanced calcium homeostasis also could protect against neurodegeneration. Down-regulation of L-type voltage-sensitive Ca2+ channels in hippocampal neurons has been osserved in the presence of 1,25(OH)2 D3 correlating with the neuroprotective effect against excitotoxic insults [7]. Induction of neuroprotective calcium binding proteins could promote calcium homeostasis in the brain. This has been observed with the increase in parvalbumin in rat caudate putamen in response to vitamin D treatment [17]. Another vitamin D associated cytosolic protein, calbindin- D (28k), has also been found to regulate intra-cellular calcium concentration in neurons, and shows reduced levels in the hippocampal tissue in Alzheimer’s patient [18].
Additionally, vitamin D plays a role in the cerebral processes of detoxification by interacting with reactive oxygen and nitrogen species, especially in case of excessive entry of calcium into brain neurons [5]. Calcium not stored in the endoplasmic reticulum causes the activation of nitric oxide (NO) synthase and the synthesis of NO or the stimulation of phospholipase A2, the generation of superoxide anion (O2-) [19, 20]. NO can interact with O2- to form peroxynitrite (OONO –) . Oxy-reduction reactions resulting from free radicals induce dose- dependent neuronal damage to deoxyribonucleic acid, membrane lipid by peroxidation, and enzyme inactivation. The consequences are cell contraction, relocation of organules, condensation of chromatin, nuclear fragmentation, and production of apoptotic bodies containing fragments of cytoplasm and kernel, that defines neuronal apoptosis [19, 20]. The action of detoxification of vitamin D was described on cultured rat mesencephalic cells, with an efficient protection against the superoxide ion, hydrogen peroxide, and intracellular free radicals generated by reactive oxygen species (ROS) [21].
In addition, it has been demonstrated that vitamin D inhibits the synthesis of inducible nitric oxide synthase (NOS), an enzyme produced in the Central Nervous System (CNS) cells in response to stress, the high-dose action of which results in neuronal cell alteration [14]. The consequence of vitamin D administration is an increase in the number of survival neurons after exposure to cytotoxic stimuli. Another relatively direct effect could be through increased neurotrophin synthesis (NGP), as suggest at finding that 1,25(OH)D stimulate synthesis of nerve growth factor glial cell line derived neurotropic factor (GDNF) and neurotrophin (NT3) in varius non clinical studies [22-26]. Vitamin D-related trophic induction seems to play a neuroprotective role in cerebral ischemia as well as an antineurodegenerative role for dopaminergic cells in experimental animal models of Parkinson’s disease [14, 22, 27].
Finally, a more direct effect might derive through the increase in acetylcholine concentrations in the brain (CAT), as suggested by the finding that 1,25 (OH)2 D3 treatment incrementes choline acetyltransferase activity in specific rat brain nuclei [28]. CAT Keys a remorkable role in acetilcholine synthesis (Ach).
Conclusion
Our results showed a relationship between 25(OH)D and cognitive impairment in patients with AD, suggesting that 25(OH)D could be involved in the onset of dementia. Clearly, an association between low vitamin D status and cognitive impairment does not establish that vitamin D deficiency causes cognitive impairment. Additional investigatation of this clinical observation, particularly with intervention al studies, is closely requested.
Funding
None.
Conflicts of Interest
None.
