The Anaesthetic Management of a Parturient with an Ebstein Anomaly and Prior Bidirectional Glenn Shunt
A B S T R A C T
Parturients with Ebstein anomaly are an anaesthetic challenge due to the spectrum of disease. Patients palliated with bidirectional Glenn shunts are susceptible to right heart dysfunction due to the physiological changes during parturition. We present a 28-year-old primigravida with Ebstein anomaly surgically managed by a bidirectional Glenn shunt. Echocardiograms showed normal right ventricular function despite reported dyspnea as the pregnancy progressed. Following a comprehensive plan developed during multidisciplinary prenatal meetings, she safely delivered. In this case report, we discuss the preoperative evaluation, management of labour and delivery, and postpartum planning of parturients with palliated Ebstein anomaly.
Keywords
Ebstein anomaly, Glenn shunt, obstetric anaesthesiology, pregnancy
Introduction
Ebstein anomaly is a congenital malformation with atrialization of the right ventricle (RV). The tricuspid valve (TV) septal leaflet is apically displaced in a small RV and a large right atrium (RA) (Figure 1) [1]. The TV deformity leads to tricuspid regurgitation (TR), arrhythmias, and right heart failure (HF). Most patients are asymptomatic, but those with severe abnormalities often require surgical treatment [2, 3]. Severe RV dilation and systolic dysfunction are an indication for a bidirectional Glenn shunt procedure [4]. Despite surgical interventions, the physiologic changes of pregnancy place these patients at high risk of HF [5]. Prior reports have presented the peripartum management of patients with unrepaired Ebstein anomaly [3-5]. This case report describes the anaesthetic management of a parturient with a history of Ebstein anomaly palliated with a bidirectional Glenn shunt [5-7]. The patient gave written HIPAA authorization.
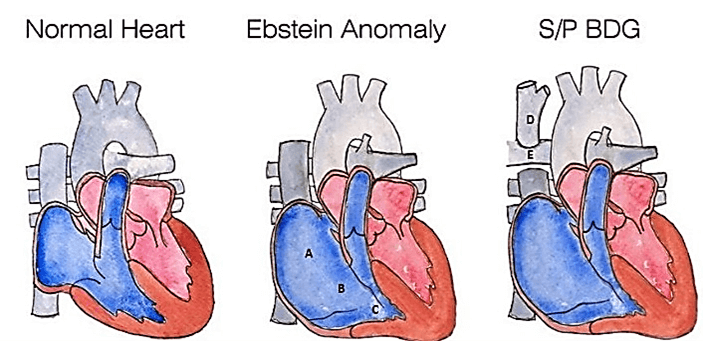
Figure 1: The first image is of normal cardiac anatomy. The second image is of the Ebstein anomaly demonstrating A) an enlarged right atrium apically displaced, B) an enlarged tricuspid valve and C) a residual right ventricle. The third image shows the bidirectional Glenn shunt [D) the superior vena cava anastomosed to E) the right pulmonary artery].
Case Report
A 28-year-old female G1P0 at 38 weeks presented for induction of labour. At the age of 19, she was diagnosed with severe Ebstein anomaly complicated by a large atrial septal defect (ASD) and right HF. She underwent a bidirectional Glenn shunt with ASD fenestrated patch closure and TV repair. The bidirectional Glenn procedure entails disconnecting the superior vena cava (SVC) from the RA and anastomosing it to the right pulmonary artery (Figure 1) [8]. When the patient initially presented at 8 weeks gestation, the obstetrician advised termination, but the patient chose to continue her pregnancy. The transthoracic echocardiogram (TTE) at that time demonstrated a small ASD, large RA, small RV, mild-moderate TR, and normal biventricular function.
As her pregnancy progressed, she experienced dyspnea, orthopnea, and cyanosis, but her third trimester TTE remained unchanged. A group of specialists consisting of cardiologists, intensivists, maternal-fetal medicine specialists, and obstetric anaesthesiologists formulated a careful plan for delivery. An induction with trial of labour under neuraxial anaesthesia in the labour and delivery suite was determined to be the best plan. Initial vital signs were a heart rate of 89 beats/min, blood pressure of 112/66 mmHg, respiratory rate of 18/min, and an oxygen saturation of 94% on room air. After preoperative evaluation, an arterial line was placed for close hemodynamic monitoring followed by dural puncture epidural at the L4-L5 level prior to onset of pain. After a negative test dose, an infusion of 0.0625% bupivacaine plus fentanyl 2 mcg/mL was started at 6 mL/hour without bolusing and slowly titrated up to a rate of 12 mL/hour while monitoring hemodynamics, symptoms, and fetal heart rate. A dural puncture epidural is a modification of the combined spinal-epidural technique, where the dura is perforated with a 25G or 26G spinal needle but intrathecal medications are not administered. No intravenous fluid was bolused.
The risk of deep vein thromboembolism (DVT) was determined to be low and sequential compression devices were used. The obstetric team induced labour with misoprostol and a cervical foley with oxytocin augmentation. A dual nursing team from labour and delivery and the cardiac care unit (CCU) continuously monitored electrocardiography and hemodynamics during labour. Pain was well controlled with consistent patient-reported pain scores of less than 5 on a scale of 1 to 10. She safely delivered with Apgar scores of 9 and 9. The patient was administered tranexamic acid and Methergine. Postpartum blood loss was 550 mL. She was transferred to the CCU for postpartum care where she experienced lightheadedness and fatigue and was found to have a haemoglobin of 8 g/dL. She was transfused one unit of packed red blood cells for symptomatic anemia with subsequent resolution of symptoms. She was discharged on postpartum day 3.
Discussion
Ebstein anomaly consists of a large RA and small RV due to failure of delamination of the TV leaflets and can affect up to 0.005% of live births [4, 9]. Associated malformations include ASD, ventricular septal defect, pulmonary stenosis, patent ductus arteriosus, and RV outflow tract obstruction [10]. Other anomalies include low-set ears, micrognathia, cleft lip, cleft palate, absent left kidney, and megacolon. Because of RA dilation, these patients are at risk for supraventricular arrhythmias, anomalous atrioventricular conduction pathways, and Wolff-Parkinson-White syndrome [9]. The clinical severity of Ebstein anomaly is a spectrum ranging from death in utero to incidental findings in asymptomatic adults. Management mostly consists of surveillance and medical optimization. Surgical delay until the development of HF is associated with worse outcomes [4]. Surgical treatment ranges from TV repair to a Fontan procedure. Our patient had developed severe TR and RV dysfunction, and subsequently underwent a bidirectional Glenn procedure to reduce RV volume overload and improve RV function, resulting in improved exercise tolerance and quality of life.
The bidirectional Glenn procedure entails disconnecting the SVC from the RA and anastomosing it to the right pulmonary artery (Figure 1) [8]. This reduces RV preload and workload while oxygenation and LV cardiac output are maintained. Commonly, these patients have normal oxygen saturations as seen in our patient’s vitals, but desaturation may occur with right-to-left shunting. Similarly, our patient had developed cyanosis from shunting across her ASD during early pregnancy likely due to increases in blood volume. Blood flow through the bidirectional Glenn shunt is dependent on pulmonary vascular resistance. Factors that increase pulmonary vascular resistance, such as labour pain and hypoxia, will decrease flow through the shunt. Physiologic hemodynamic changes of pregnancy, including increased blood volume and pulmonary vascular resistance, pose significant risk for right HF. Pregnancy and delivery are well-tolerated in unrepaired asymptomatic patients with Ebstein anomaly [5, 6, 11, 12]. In symptomatic patients, pregnancy poses a risk for HF, worsening cyanosis, and arrhythmia [5, 11]. More than half of women with cyanosis deteriorate during pregnancy compared to just 15% of acyanotic patients, and maternal mortality is 30% in those with pulmonary hypertension [13, 14]. Maternal risk is theoretically reduced after surgical repair or catheter ablation of accessory pathways [6]. Despite this, some experts still advise against pregnancy [1]. Our patient was advised to terminate her pregnancy due to her complex congenital disease and elevated risk for developing symptomatic HF.
A multidisciplinary team consisting of obstetricians, anaesthesiologists, cardiologists, intensivists, and nurses is key to the safe management of these high-risk patients. A baseline TTE early in pregnancy should be obtained with the frequency of monitoring determined by a cardiologist experienced in caring for patients with congenital heart disease [5]. Pregnancy is a procoagulant state and bidirectional Glenn shunt patients are deficient in both pro- and anticoagulant factors [15]. Cardiologists and hematologists should determine the risk of thromboembolism and bleeding to guide DVT prophylaxis. Management ranges from compression devices to anticoagulants. The optimal location for labour, delivery, and recovery should be determined after multidisciplinary discussion taking into consideration the severity of the patient’s symptoms, proximity to the CCU, and the clinical experience of the institution. Our CCU is on a different floor from the operating room requiring transport via an elevator in case of an emergency cesarean section. In addition, our labour and delivery nurses are trained to monitor the fetal heart tracing.
Thus, the labour and delivery suite was chosen for induction of labour instead of the CCU. The patient is at high risk of HF and arrhythmias in the peripartum period, and the risk is highest after delivery due to the effects of auto-transfusion. Thus, we decided on recovering the patient in the CCU. Vaginal delivery with neuraxial anaesthesia is our preferred delivery plan. Epidural placement followed by a titrated infusion is recommended before induction of labour to allow time for adequate analgesia. We performed a dural puncture epidural followed by a slow infusion to avoid an abrupt sympathectomy. It is postulated that this technique decreases the time of onset and improves caudal spread of analgesia compared with the epidural technique without the sympathectomy observed with the combined spinal epidural technique [16, 17].
Fluid management is guided by the patient’s volume status as maintaining clinical euvolemia is crucial. Strict fluid monitoring in patients with Ebstein anomaly and bidirectional Glenn shunt is important to provide adequate filling pressures and avoid fluid overload. Invasive monitoring with central venous catheters is unreliable because the SVC reflects pulmonary artery pressures, and femoral venous pressures are confounded by uterine compression of the vena cava. TTE is useful to monitor cardiovascular function and volume status. Bedside TTE was available in the event of sudden decompensation. Minor changes including chamber dilatation, a normal to midline interventricular septum, and increases in TV gradients are anticipated [5]. A patient bidirectional Glenn shunt and minimal ventilatory changes in the caval diameter are desired endpoints. RA filling pressure should be maintained at higher than normal levels in the presence of TR and elevated RV pressure, as seen in our patient [11]. During and immediately following delivery, increases in venous return from auto-transfusion and vena caval decompression may cause RV volume overload, right HF, and low cardiac output. This can be seen on TTE with the septum bulging into the LV with RV dilation [11]. Fortunately, the bidirectional Glenn shunt provides limited RV preload as long as the pulmonary vascular resistance remains low.
Conclusion
Surgically palliated Ebstein anomaly has led to improved survival and quality of life, resulting in more and more patients presenting for obstetric care [4]. The physiologic changes of pregnancy present a unique challenge in the safe anaesthetic management of this patient population. Successful clinical management requires a comprehensive understanding of the pathophysiology of the associated cardiac lesions and implications of prior surgical repairs. Obstetric care should be planned at a high-risk center led by a multidisciplinary team of specialists. A plan for frequent imaging and mode of delivery will inform a carefully crafted anaesthetic plan. Neuraxial anaesthesia may be preferred. A critical care team who is prepared to receive the patient will help optimize the postpartum management of the mother to help ensure a good outcome.
Acknowledgment
None.
Conflicts of Interest
None.
Article Info
Article Type
Case ReportPublication history
Received: Mon 31, May 2021Accepted: Sat 14, Aug 2021
Published: Thu 19, Aug 2021
Copyright
© 2023 Shamantha G. Reddy. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2021.08.08
Figures & Tables
References
1. Resnik R, Lockwood
CJ, Moore TR, Greene MF, Copel J et al. (2019) Creasy and Resnik's
Maternal-Fetal Medicine: Principles and Practice. Medicine 55: 920-948.
2.
Bove EL, Hirsch JC, Ohye RG, Devaney EJ (2009) How I
manage neonatal Ebstein's anomaly. Semin Thorac Cardiovasc Surg Pediatr Card
Surg Annu 63-65. [Crossref]
3. Sharma N, Lalnunnem TJ, Nandwani M, Santa SA, Synrang BW et al. (2018) Ebstein
Anomaly with Pregnancy: A Rare Case. J Reprod Infertil 19: 119-122. [Crossref]
4. Stout KK, Daniels
CJ, Aboulhosn JA, Bozkurt B, Broberg CS et al. (2019) 2018 AHA/ACC Guideline
for the Management of Adults With Congenital Heart Disease: A Report of the
American College of Cardiology/American Heart Association Task Force on
Clinical Practice Guidelines. Circulation 139: e698-e800. [Crossref]
5. Regitz Zagrosek V,
Roos Hesselink JW, Bauersachs J, Blomström Lundqvist C, Cífková R et al. (2018)
2018 ESC Guidelines for the management of cardiovascular diseases during
pregnancy. Eur Heart J 39: 3165-3241. [Crossref]
6.
Connolly
HM, Warnes CA (1994) Ebstein's anomaly: outcome of pregnancy. J Am Coll
Cardiol 23: 1194-1198. [Crossref]
7.
Donnelly JE, Brown JM, Radford DJ (1991) Pregnancy
outcome and Ebstein's anomaly. Br Heart J 66: 368-371. [Crossref]
8. Ungerleider R,
Meliones JN, McMillan KN, Cooper DS, Jacobs JP et al. (2019) Critical Heart
Disease in Infants and Children.12: 108-109.
9. Knott Craig CJ,
Goldberg SP, Ballweg JA, Boston US (2012) Surgical Decision Making in Neonatal
Ebstein's Anomaly: An Algorithmic Approach Based on 48 Consecutive Neonates. World
J Pediatr Congenit Heart Surg 3: 16-20. [Crossref]
10. Kogon BE, Plattner
C, Leong T, Simsic J, Kirshbom PM et al. (2008) The bidirectional Glenn
operation: a risk factor analysis for morbidity and mortality. J Thorac
Cardiovasc Surg 136: 1237-1242. [Crossref]
11. Canobbio MM, Warnes
CA, Aboulhosn J, Connolly HM, Khanna A et al. (2017) Management of Pregnancy in
Patients With Complex Congenital Heart Disease: A Scientific Statement for
Healthcare Professionals From the American Heart Association. Circulation 135:
e50-e87. [Crossref]
12. Drenthen W, Pieper
PG, Roos Hesselink JW, van Lottum WA, Voors AA et al. (2007) Outcome of
pregnancy in women with congenital heart disease: a literature review. J Am
Coll Cardiol 49: 2303-2311. [Crossref]
13. Shime J, Mocarski
EJ, Hastings D, Webb GD, McLaughlin PR et al. (1987) Congenital heart disease
in pregnancy: short- and long-term implications. Am J Obstet Gynecol
156: 313-322. [Crossref]
14. Pitkin RM, Perloff
JK, Koos BJ, Beall MH (1990) Pregnancy and congenital heart disease. Ann
Intern Med 112: 445-454. [Crossref]
15. Odegard KC, McGowan
FX Jr, Zurakowski D, DiNardo JA, Castro RA et al. (2002) Coagulation factor
abnormalities in patients with single-ventricle physiology immediately prior to
the Fontan procedure. Ann Thorac Surg 73: 1770-1777. [Crossref]
16. Gunaydin B, Erel SJ (2019) How neuraxial labor analgesia differs by approach: dural puncture epidural as a novel option. J Anesth 33: 125-130. [Crossref]
17. Heesen M, Rijs K, Rossaint R, Klimek M (2019) Dural puncture epidural versus conventional epidural block for labor analgesia: a systematic review of randomized controlled trials. Int J Obstet Anesth 40: 24-31. [Crossref]