The Forgotten Ventricle: Sub-Pulmonary LV Failure in a Patient with Transposition of the Great Arteries Post Atrial Switch Repair
A B S T R A C T
We present the case of a patient with transposition of the great arteries (TGA) post atrial switch repair (Mustard) with a failing sub-pulmonary left ventricle. Our case highlights the importance of early identification of a failing sub-pulmonary LV and the significance of utilising multi-modality imaging in diagnosing and monitoring these patients. Similarly, it emphasizes the importance of a holistic approach in managing patients with complex physical and psychological needs in relation to timely transplantation referral.
Keywords
Sub-pulmonary LV, systemic RV, mustard repair, transposition of the great arteries, heart failure, atrial switch operation
History of Presentation
A 48-year-old male with a past medical history of a Mustard repair for TGA, recurrent decompensated heart failure (HF) despite being on maximally tolerated HF medications and psychosocial issues, presented to his local hospital with worsening breathlessness on the background of NYHA function class II. He had rapid deterioration in exercise capacity to NYHA IV, significant weight loss, abdominal pain and nausea. Clinical Timelines are detailed in (Table 1).
Investigations
On admission, his routine bloods confirmed renal and liver impairment with worsening BNP (Tables 1 & 2). ECG showed sinus rhythm consistent with systemic Right ventricular (sRV) hypertrophy and chest x-ray showed cardiomegaly (Figure 1). Transthoracic Echocardiography (TTE) showed the systemic and pulmonary venous baffles were unobstructed with no obvious baffle leak. As was shown previously, the sRV was significantly dilated and hypertrophied (Figure 2, Table 3, Video 1 & Video 2) with moderately reduced systolic function (Figure 3). The pulmonary venous atrium and tricuspid annulus remained severely dilated, resulting in tethering of the leaflets with failure of coaptation and severe tricuspid regurgitation (TR) (Figure 2, Video 3).
Most importantly, there was significant dilatation and deterioration of the sub-pulmonary LV systolic function (2D Biplane EF 24%), which was normal in size and function less than 4 months previously (Figure 3). There was an echogenic mass in the LV apex (1.6×1.4 cm) suggestive of thrombus (Table 3, Figure 4, Video 4). There was trivial mitral valve regurgitation with peak velocity 3.5 m/s and calculated pressure gradient of 50 mmHg, estimated pulmonary artery systolic pressure 65 mmHg considering a systemic venous atrial pressure of 15 mmHg (Figure 5). From early pulmonary regurgitation velocity, calculated mean pulmonary artery pressure (mPAP) was 49 mmHg. The inferior vena cava was significantly dilated, poor respiratory variability and a large atrial reversal of hepatic vein flow (Figure 6).
Table 1: Timeline of patient history prior to admission.
|
Time |
Events |
BNP (ng/L) |
Investigation |
|
1972 |
Rashkind Balloon Atrial
septostomy |
|
|
|
1974 |
Mustard operation |
|
|
|
2014 |
First admission with
decompensated acute heart failure. |
|
|
|
2017 |
Admission for decompensated heart failure. Self-discharged. Future heart transplantation discussed.
|
168 |
|
|
2019 |
Admission for decompensated
heart failure Continues to smoke Offered heart transplantation
assessment |
134
|
|
|
June 2020 |
Admitted with: ·
decompensated biventricular heart failure ·
renal and
liver dysfunction ·
LV thrombus Deemed unsuitable for heart transplantation Self-discharged
|
1457 |
|
|
July 2020 |
Readmitted with: ·
decompensated heart failure ·
acute liver injury ·
LV thrombus resolved. Guarded prognosis - referred to
Palliative Community care. Self-discharged again |
|
|
|
August 2020 |
Admitted locally with: • peritonitis • CT suggestive of
bowel perforation. • Emergency laparotomy
showed no perforation but likely pancreatitis. • Decompensated heart
failure • Renal and Liver
dysfunction
Patient Deceased – most likely sudden cardiac death |
|
LVEF 15%. Severely dilated RV, severe TR |
Table 2: Admission blood results.
|
Blood Test |
Value |
Normal range |
|
Haemoglobin |
12.1 g/L |
13.4-16.6 |
|
White cell count |
6.9 X109/L |
4.4-10.1 |
|
CRP |
|
|
|
Sodium |
123 mmol/L |
133-146 |
|
Potassium |
3.5mmol/L |
3.5-5.3 |
|
Urea |
6.8 mmol/L |
2.5-7.8 |
|
Creatinine |
111
umol/L |
60-120 |
|
Estimated GFR |
62 ml/min |
|
|
Bilirubin |
57umol/L |
0-20 |
|
ALP |
183 U/L |
30-130 |
|
ALT |
255
IU/L |
8-40 |
|
Total protein |
57 g/L |
60-80 |
|
BNP |
1225 ng/L |
0-20 |
Table 3: TTE parameter comparisons.
|
Measurement |
|
Admission
(22/06/2020) |
<4
months prior admission (09/03/2020) |
TR
became severe (2017) |
Moderate
TR (2016) |
|
Systemic
RV |
Size |
Dilated |
Dilated |
Dilated |
Dilated |
|
Basal
(mm) |
56 |
58 |
4.3 |
53 |
|
|
Mid
(mm) |
50 |
54 |
3.5 |
46 |
|
|
Function |
Impaired |
Impaired |
Impaired |
Impaired |
|
|
TAPSE
(mm) |
9 |
7 |
13 |
7 |
|
|
RV
S’ (cm/s) |
6 |
6 |
5 |
4 |
|
|
FAC
(%) |
30 |
21 |
26 |
23 |
|
|
RA |
Size |
Dilated |
Dilated |
Dilated |
Dilated |
|
Volume
(ml/m2) |
63.9 |
56 |
26.8
cm2 |
27.5
cm2 |
|
|
TV
annulus |
Size |
Dilated |
Dilated |
Dilated |
Dilated |
|
Diameter
(cm) |
4.3 |
4.8 |
4.5 |
4.5 |
|
|
TR
severity |
Semi-quantitative
|
Severe |
Severe |
Severe |
Moderate |
|
Pulmonic
LV
|
Size |
Dilated |
Normal
size |
Normal
size |
Normal
size |
|
LVEDd
(cm) |
5.8 |
4.3 |
4.5 |
4.4 |
|
|
Function |
Impaired |
Normal
function |
Normal
function |
Normal
function |
|
|
Biplane
EF (%) |
24 |
visually |
Visually |
visually |
|
|
FAC
(%) |
8 |
46 |
33 |
44 |
|
|
MR |
Qualitative
Degree |
Trivial |
No
MR |
No
MR |
No
MR |
|
Hemodynamics |
|
|
|
||
|
Velocity
(m/s) |
3.5 |
-- |
-- |
-- |
|
|
PG
(mmHg) |
50 |
-- |
-- |
-- |
|
|
LVSP
(mmHg) |
65 |
-- |
-- |
-- |
|
|
PR |
Qualitative
Degree |
Trivial |
Trivial |
Trivial |
Trivial |
|
Hemodynamics |
|
|
|
||
|
PAP
(mmHg) |
49 |
-- |
-- |
-- |
|
TAPSE: Tricuspid Annular Plane Systolic
Excursion; FAC: Fractional Area Change; RA: Right Atrium; LVEDd: Left
Ventricular End-Diastolic diameter; PG: Peak Gradient, EF: Ejection Fraction;
LVSP: Left Ventricular Systolic Pressure; PAP: Pulmonary Artery Pressure.

Figure 1: A) ECG features of Systemic RV – flat p waves, RV hypertrophy (increased RV electrical forces anteriorly). Small R wave and deep S waves in left precordial leads. B) CXR showing PICC line in SVC, the heart is enlarged. Prominent pulmonary arteries, particularly the right main PA at the right hilum and pulmonary vasculature in the left upper lobe, which is slightly more prominent than on the previous radiograph.
Dual acquisition computed tomography coronary angiogram (CTCA) and CT pulmonary angiography (CTPA) confirmed the LV thrombus with no evidence of LV infarction or pulmonary embolus (Figure 5). Abdominal ultrasound was consistent with HF - dilated hepatic veins, periportal oedema with hepatic and portal vein spectral waveforms and the presence of small volume peri-hepatic free fluid and an oedematous gallbladder. Additionally, lung function tests showed a moderate reduction in vital capacity but no evidence of significant airway obstruction.
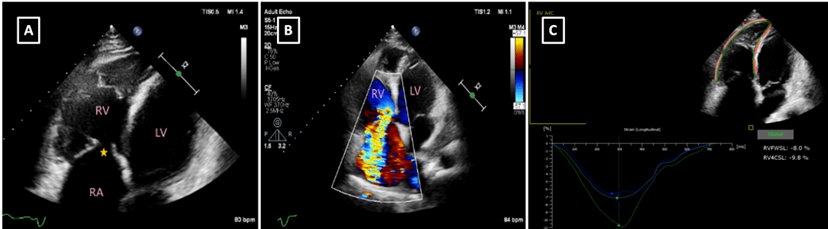
Figure 2: A) Apical 4-chambers view. LV: sub-pulmonary LV, RA: right atrium, RV: right ventricle, star: deficient leaflets coaptation B) Apical 4-chambers view with colour Doppler showing severe/free TR. (VC 1.2 cm, PISA radius 1.4 cm, PISA EROA 1.8 cm²; RV 109 ml). RV: systemic RV, LV: sub-pulmonary LV C) Apical 4-chambers view. Calculation of systemic RV GLS –9.8% and RV free wall LS –8%.
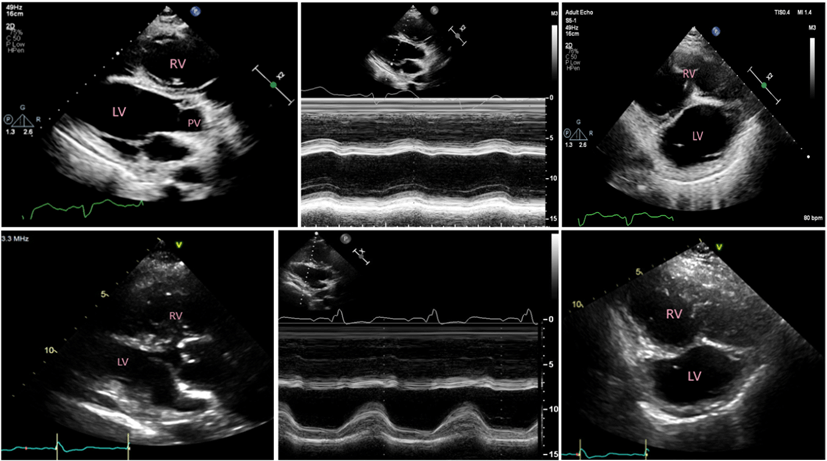
Figure 3: Top panel from left to right (parasternal long axis, M-mode and parasternal short axis) showing dilated and impaired sub-pulmonary LV. Bottom panel: similar views from 4 months prior showing preserved sub-pulmonary LV size and function.
A right heart catheter showed a mean pulmonary arterial pressure of 45mmHg, PCWP (systemic venous atrial pressure) 15mmHg, sub-pulmonary LV EDP 6mmHg, Cardiac Output (CO) 3.35L/m2, CI 1.79, PVR 8.9 Woods units. After sodium Nitroprusside PA mean 16mmHg, PCWP 3mmHg, CO 6.6L/m2, PVR 1.97 Woods unit. In summary, our 48-year-old patient presented with decompensated HF and worsening pulmonary hypertension (PH). His liver impairment and renal dysfunction are highly likely due to the increased venous pressure and low cardiac output.
Management
The patient was commenced on a furosemide infusion with fluid restriction, intravenous heparin, ionotropes, and optimization of HF medications. In parallel, assessment for heart transplantation was re-instigated. Due to prolonged hospitalization without visitors as COVID restrictions, he expressed frustration and eventually self-discharged, despite emphasizing the risk of ventricular arrythmia and SCD without an ICD in situ (he was thought to be a good candidate for primary prevention ICD). He was subsequently deemed unsuitable for heart transplantation or ventricular assist device (VAD) as destination therapy in view of his PH, psychosocial concerns and history of non-compliance with medications in the past. He was therefore referred to community palliative care with a guarded prognosis. He was seen locally two months later with acute abdomen distension and HF symptoms and died during the course of his admission.
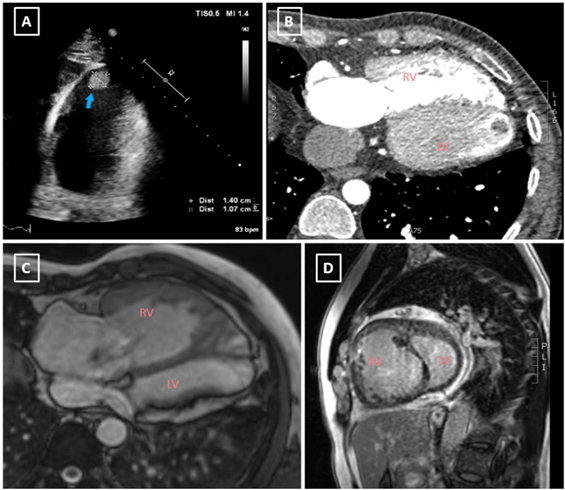
Figure 4: A) TTE showing sub-pulmonary LV apical thrombus B) Contrast CT confirming dilated sub-pulmonary LV with apical thrombus. Bottom panel: C & D) CMR demonstrating appropriately small sub-pulmonary LV from 2017.
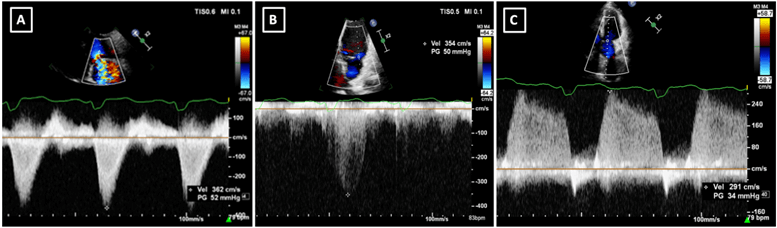
Figure 5: A) Tricuspid inflow view. TR jet from CW Doppler, B) Apical 4 chambers view. Jet of MR from CW Doppler, C) Pulmonary flow CW Doppler spectral signal. Estimation of mean pulmonary artery pressure (49mmHg).
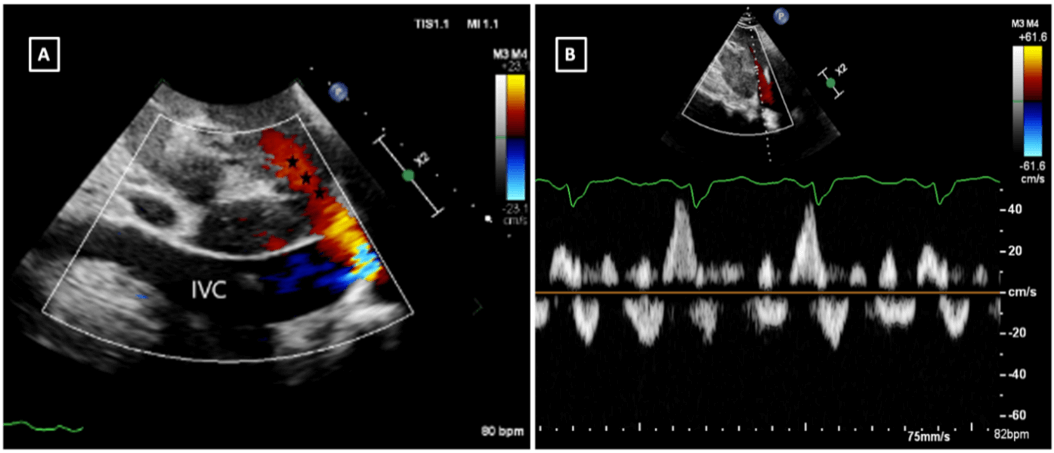
Figure 6: A) Dilated IVC (2.9cm) and hepatic vein with the large reverse flow in the hepatic vein (Asterixis). B) PW Doppler demonstrated significant flow reversal in hepatic veins.
Discussion
Systemic RV failure and the development of TR are common in adult patient with TGA after Mustard repair. Failing of the sub-pulmonary LV has not yet been seen in the majority of patients in this population. The combination of pulmonary hypertension and LV failure with multi-organ failure has been the cause of death in this patient. TGA is a complex cyanotic congenital heart disease where the systemic and pulmonary circulations run in parallel. The atrial switch procedure (Mustard repair) was performed by creating baffles and re-routing venous flow to the concordant side of the heart, resulting in a morphological RV supporting the systemic circulation. Thus, being subjected to systemic pressures results in RV hypertrophy, dilatation and dysfunction, which develops over time. Subsequently, functional tricuspid regurgitation secondary to RV dysfunction is often seen in older patients, which is expected in approximately 50% of patients in the 5th Decade [1]. This is opposed to left ventricular dysfunction and significant mitral regurgitation, which are unusual in this setting.
Normally, the sub-pulmonary LV becomes smaller as a result of deconditioning, remodelling and adapting to low pulmonary pressures (Figure 4, Video 5), rendering it unable to withstand an increase in pulmonary pressure later in life [2]. Our patient presented with sub-pulmonary LV dilatation, dysfunction and thrombus. Sub-pulmonary LV and sRV systolic pressure were equal in the absence of pulmonary stenosis, possibly secondary to the development of PH. Other potential causes of sub-pulmonary LV dysfunction had to be excluded, such as atherosclerosis, and emboli to the coronary and pulmonary arteries. This is a critical situation where urgent transplant and/or VAD insertion should be considered. Other expected complications include arrythmias and atrial baffle leaks or obstruction, which were ruled out by TTE [3].
Pulmonary hypertension in TGA Mustard patients is of two types: one (more common) is pre-capillary and the other is post-capillary. It is important to use PR velocity to identify increased PA pressure in the absence of mitral regurgitation (mPAP) [3]. Also, LV dilatation with septal flattening are indirect sign of increased LV pressure (the usual bullet-shaped LV is abnormal in this setting). Evidence pointing towards PH, in this case, is the MV regurgitation velocity being equal to the TV regurgitation. Considering the patient’s systolic BP and gradient across the TV, and increased pulmonary venous atrial pressure of 38 mmHg was calculated and suggesting a significantly elevated PCWP (Table 3). Reduction of ventricular compliance leads to an increase in end-diastolic pressures and consequent increase in atrial and PCWP, likely resulting in PH. The increase in atrial pressure leads to chamber dilatation and increases the risk of arrhythmia [3, 4]. HF is a leading cause of mortality and morbidity in ACHD, accounting for 21-40% of all ACHD deaths [2, 4]. Sub-pulmonary LV systolic dysfunction is independently and more significantly associated with NYHA class III- IV than sRV dysfunction [2]. LV FAC has higher sensitivity and specificity in differentiating between patients in NYHA class I-II vs. III- IV compared to sRV. LV failure with thrombus formation is very rare, indicating end-stage disease.
Conclusion
This case is unique in highlighting the rare occurrence of a large apical thrombus in a failing, dilating sub-pulmonary LV secondary to the development of PH after Mustard repair presenting with decompensated HF. This represents end-stage disease. The sRV was dilated and impaired as expected with functional TR. Adverse ventriculo-ventricular interaction and excessive total ventricular mass have been proposed in this setting and may have been operational here. We also discuss the challenges of early identification of HF in ACHD patients at risk and adopting a holistic approach to their management with complex physical and psychological needs and timely introduction of cardiac transplantation.
Conflicts of Interest
None.
Funding
None.
Abbreviation
BNP: Brain Natriuretic Peptide
CO: Cardiac Output
HF: Heart Failure
ICD: Implantable Cardiac Defibrillator
LV: Left Ventricle
PCWP: Pulmonary Capillary Wedge Pressure
PH: Pulmonary Hypertension
SCD: Sudden Cardiac Death
sRV: Systemic Right Ventricle
TGA: Transposition of the Great Arteries
TR: Tricuspid Regurgitation
TTE: Transthoracic Echocardiography
Article Info
Article Type
Case ReportPublication history
Received: Tue 12, Jul 2022Accepted: Fri 29, Jul 2022
Published: Thu 08, Sep 2022
Copyright
© 2023 Nada Al-Sakini. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.IJSCR.2022.01.05
Figures & Tables
Table 1: Timeline of patient history prior to admission.
|
Time |
Events |
BNP (ng/L) |
Investigation |
|
1972 |
Rashkind Balloon Atrial
septostomy |
|
|
|
1974 |
Mustard operation |
|
|
|
2014 |
First admission with
decompensated acute heart failure. |
|
|
|
2017 |
Admission for decompensated heart failure. Self-discharged. Future heart transplantation discussed.
|
168 |
|
|
2019 |
Admission for decompensated
heart failure Continues to smoke Offered heart transplantation
assessment |
134
|
|
|
June 2020 |
Admitted with: ·
decompensated biventricular heart failure ·
renal and
liver dysfunction ·
LV thrombus Deemed unsuitable for heart transplantation Self-discharged
|
1457 |
|
|
July 2020 |
Readmitted with: ·
decompensated heart failure ·
acute liver injury ·
LV thrombus resolved. Guarded prognosis - referred to
Palliative Community care. Self-discharged again |
|
|
|
August 2020 |
Admitted locally with: • peritonitis • CT suggestive of
bowel perforation. • Emergency laparotomy
showed no perforation but likely pancreatitis. • Decompensated heart
failure • Renal and Liver
dysfunction
Patient Deceased – most likely sudden cardiac death |
|
LVEF 15%. Severely dilated RV, severe TR |
Table 2: Admission blood results.
|
Blood Test |
Value |
Normal range |
|
Haemoglobin |
12.1 g/L |
13.4-16.6 |
|
White cell count |
6.9 X109/L |
4.4-10.1 |
|
CRP |
|
|
|
Sodium |
123 mmol/L |
133-146 |
|
Potassium |
3.5mmol/L |
3.5-5.3 |
|
Urea |
6.8 mmol/L |
2.5-7.8 |
|
Creatinine |
111
umol/L |
60-120 |
|
Estimated GFR |
62 ml/min |
|
|
Bilirubin |
57umol/L |
0-20 |
|
ALP |
183 U/L |
30-130 |
|
ALT |
255
IU/L |
8-40 |
|
Total protein |
57 g/L |
60-80 |
|
BNP |
1225 ng/L |
0-20 |
Table 3: TTE parameter comparisons.
|
Measurement |
|
Admission
(22/06/2020) |
<4
months prior admission (09/03/2020) |
TR
became severe (2017) |
Moderate
TR (2016) |
|
Systemic
RV |
Size |
Dilated |
Dilated |
Dilated |
Dilated |
|
Basal
(mm) |
56 |
58 |
4.3 |
53 |
|
|
Mid
(mm) |
50 |
54 |
3.5 |
46 |
|
|
Function |
Impaired |
Impaired |
Impaired |
Impaired |
|
|
TAPSE
(mm) |
9 |
7 |
13 |
7 |
|
|
RV
S’ (cm/s) |
6 |
6 |
5 |
4 |
|
|
FAC
(%) |
30 |
21 |
26 |
23 |
|
|
RA |
Size |
Dilated |
Dilated |
Dilated |
Dilated |
|
Volume
(ml/m2) |
63.9 |
56 |
26.8
cm2 |
27.5
cm2 |
|
|
TV
annulus |
Size |
Dilated |
Dilated |
Dilated |
Dilated |
|
Diameter
(cm) |
4.3 |
4.8 |
4.5 |
4.5 |
|
|
TR
severity |
Semi-quantitative
|
Severe |
Severe |
Severe |
Moderate |
|
Pulmonic
LV
|
Size |
Dilated |
Normal
size |
Normal
size |
Normal
size |
|
LVEDd
(cm) |
5.8 |
4.3 |
4.5 |
4.4 |
|
|
Function |
Impaired |
Normal
function |
Normal
function |
Normal
function |
|
|
Biplane
EF (%) |
24 |
visually |
Visually |
visually |
|
|
FAC
(%) |
8 |
46 |
33 |
44 |
|
|
MR |
Qualitative
Degree |
Trivial |
No
MR |
No
MR |
No
MR |
|
Hemodynamics |
|
|
|
||
|
Velocity
(m/s) |
3.5 |
-- |
-- |
-- |
|
|
PG
(mmHg) |
50 |
-- |
-- |
-- |
|
|
LVSP
(mmHg) |
65 |
-- |
-- |
-- |
|
|
PR |
Qualitative
Degree |
Trivial |
Trivial |
Trivial |
Trivial |
|
Hemodynamics |
|
|
|
||
|
PAP
(mmHg) |
49 |
-- |
-- |
-- |
|
TAPSE: Tricuspid Annular Plane Systolic
Excursion; FAC: Fractional Area Change; RA: Right Atrium; LVEDd: Left
Ventricular End-Diastolic diameter; PG: Peak Gradient, EF: Ejection Fraction;
LVSP: Left Ventricular Systolic Pressure; PAP: Pulmonary Artery Pressure.
References
1.
Brida
M, Diller G, Gatzoulis MA (2018) Systemic Right Ventricle in Adults With
Congenital Heart Disease. Anatomic and Phenotypic Spectrum and Current Approach
to Management. Circulation 137: 508-518. [Crossref]
2.
Surkova
E, Segura T, Dimopoulos K, Bispo D, Flick C et al. (2021) Systolic dysfunction
of the subpulmonary left ventricle is associated with the severity of heart
failure in patients with a systemic right ventricle. Int J Cardiol 324:
66-71. [Crossref]
3. Van De Bruaene A, Toh N, Hickey EJ, Benson L, Horlick E et al. (2019) Pulmonary hypertension in patients with a subaortic right ventricle: prevalence, impact and management. Heart 105: 1471-1478. [Crossref]
4. Diller G, Kempny A, Alonso Gonzalez R, Swan L, Uebing A et al. (2015) Survival Prospects and Circumstances of Death in Contemporary Adult Congenital Heart Disease Patients Under Follow-Up at a Large Tertiary Centre. Circulation 132: 2118-2125. [Crossref]