Journals
The Great Imposture: Eosinophilic Cholangitis
A B S T R A C T
Eosinophilic Cholangitis (EC) is a rare, benign disease often mistaken for cholangiocarcinoma as clinically and radiologically EC resembles cholangiocarcinoma. Often, extensive hepatobiliary resections for a presumed malignancy are completed; however, with appropriate diagnosis EC can be managed medically. We present two cases of EC with a comprehensive literature review and a proposed diagnostic decision algorithm for EC by which to evaluate suspicious lesions with biliary obstruction and potentially avoid surgery for this benign disease.
K E Y W O R D S
biliary obstruction, benign liver disease, cholangiocarcinoma, diagnostic algorithm, malignant versus benign,
Introduction
Eosinophilic Cholangitis (EC) is described as an eosinophilic infiltrative process of the biliary tree resulting in fibrosis, stricture, obstruction and often presenting with a tumor-like appearance. EC is primarily identified as an isolated lesion and may also present with concomitant peripheral eosinophilia and/or extra-biliary involvement of the kidneys, ureters, pancreas or lymph nodes [1]. These rare lesions are often mistaken clinically and radiologically for cholangiocarcinoma, resulting in patients undergoing extensive surgical resections for presumed malignancy [2]. If a diagnosis can be confirmed, however, patients may be successfully medically managed [1].
Case Report
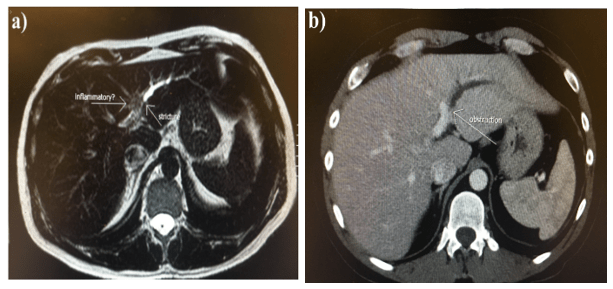
A 49-year old Caucasian male presented with epigastric/right-upper quadrant (RUQ) pain; all labs, including WBC, LFTs, AFP, CA 19-9 and CEA, were within normal limits. Eosinophil count on differential was 3.4% (normal value between 1-6%). Intrahepatic biliary stricture (Figure 1a) in the left lobe of the liver was identified on CT and an infiltrative “mass” within liver segments 4a and 4b extending into segments 2 and 3 was noted on MRI. Additionally, the obstruction and delayed contrast extravasation was noted (Figure 1b) suggesting cholangiocarcinoma and precluding any further workup. A left hepatic lobectomy with portal lymph node dissection and cholecystectomy was completed. Pathology identified a lymphocytic inflammatory cell infiltrate within the left lobe of the liver with an increased number of eosinophils. Foamy macrophages were present in the lamina propria. Additionally, in the extensive sampling of the bile ducts, fibrosis and eosinophils were present with a minimal amount of inflammation (Figure 2). Following surgery, the patient experienced an uncomplicated recovery and has remained symptom free 6-months post-op.
Our second patient is a 47-year old Caucasian female who presented with pruritis over 2-months. Total bilirubin was elevated (3.8; normal values 0.3-1.9mg/dl) as was the AST (260; normal range 10-40U/L). WBC and eosinophil (1.2%) counts were normal. CT and MRI showed severe intra-hepatic biliary dilation secondary to obstruction at the hepatic hilum. ERCP with sphincterotomy and stent placement in the common hepatic duct were completed (Figure 3) and a brush cytology was procured. Pathology identified non-diagnostic reactive ductal epithelium. Due to diagnostic uncertainty and concern for a cholangiocarcinoma, a left hepatic lobectomy with common bile duct resection and roux-en-Y hepaticojejunostomy was performed. Pathology reported a dense periductal infiltrate rich in eosinophils with associated reactive epithelial changes and periductal fibrosis along the left hepatic duct, consistent with eosinophilic cholangitis (Figure 4). At 5-year follow-up, the patient has remained disease free.



Discussion
Eosinophilic Cholangitis (EC) is a rare, benign disease of transmural eosinophilic infiltration of the biliary tree leading to stricture formation and obstruction [1, 3]. Most cases present as a focal process within the biliary system, although there have been a few reported cases of concomitant disease in the kidneys, ureters and pericardium [4]. EC was first officially reported by Leegaard et. al. in 1980, who coined the term “eosinophilic cholangitis”, and subsequently by Butler et. al. in 1985 who reported a case of a thickened gallbladder wall and stenosis of intrahepatic bile ducts with eosinophilic infiltration in the cystic duct, gallbladder, lymph nodes and bone marrow, consistent with EC [4, 5].EC is hypothesized to originate from increased IgE, IL-5 levels leading to diffuse eosinophilic infiltration of the biliary system with TGF-ß produced by eosinophils leading to fibrosis and subsequent stricture formation of the biliary tract [1, 6, 7]. While the inciting cause is unknown, EC has also been proposed as a possible extension of cholecystitis secondary to infections caused by Enterobacter aerogenes or Candida albicans [8]. A history of allergies has also been associated with peripheral eosinophilia, which may contribute to the higher incidence of EC in Western countries and Japan [9].
Studies have aimed to find a correlation between hypereosinophilic syndrome (HES), described as peripheral eosinophilia (≥1500 cells/µl for greater than 6 months) without a secondary cause, and involvement of one or more organs. However, no statistically significant correlation exists [1]. Additionally, EC may resemble primary sclerosing cholangitis (PSC), but no true association has been identified [10].
EC presents a diagnostic challenge with a differential diagnosis that includes cholangiocarcinoma, portal biliopathy, idiopathic benign focal stricture, Mirizzi syndrome, inflammatory processes secondary to choledocholithiasis, HIV cholangitis, parasitic infection, primary sclerosing cholantitis (PSC), autoimmune pancreatitis, and IgG4 cholangitis [3,6,10]. As such, it is important to exclude entities from the differential and assure appropriate treatment sequentially through appropriate imaging and laboratory testing. To facilitate a better understanding of how EC presents and begin developing a diagnostic algorithm as to appropriately exclude disease entities besides EC, the specific data points associated with each report of EC, including the two cases presented here, are detailed in Table I and summarized in Table II [1-5, 8-36].

EC typically presents in a demographic with a mean age of 42, while those younger than 40 representing the minority of cases (21%; 8/38; Table 1); males are 1.4 times more likely to develop EC as females (Tables 1 and 2). Symptoms at presentation are most often epigastric pain (24/38; 63%), jaundice (20/38; 53%) and fatigue (Tables 1 and 2) [1, 3].An examination of liver function indicators (LFTs) typically demonstrate elevated total bilirubin and complete blood count may indicate elevated eosinophil count with normal WBC (66% Table 1) however, as was seen in the two patients in our case series, the peripheral eosinophilic value may be normal (33%; Table 1) [10].
Diagnostic tests such as CEA, AFP and CA 19-9, and the autoimmune markers ASMA and ANA, have not shown to discriminate EC from any other diagnosis, suggesting limited utility [1]. Other markers, such as IgG4, which would differentiate EC from IgG4 cholangitis, may have limited utility for institutions for which this test must be sent out and may not be an expeditious option. For the cases presented here, IgG4 would not have added information which would have altered disease management.
Imaging includes abdominal CT, liver MRI and MRCP, all of which may demonstrate biliary wall thickening, biliary strictures and intrahepatic biliary dilation, with the presence of “beading” or “focal disease” more concerning for PSC or cholangiocarcinoma [2, 10]. For the cases of EC identified from the literature, imaging revealed strictures most commonly in the CBD (22/38; 58%) and IHBD (18/38; 47%; Table 1). Mass effect, proximal dilation and atrophy were not consistently documented in the literature. The two cases represented here both identified intrahepatic biliary dilation by MRI, unfortunately, imaging was not conclusive as EC and cholangiocarcinoma both often demonstrate this focal effect.
Endoscopic retrograde cholangiopancreaticogram (ERCP) can aid in diagnosis by identifying biliary strictures and allowing for specimen collection. The use of FISH (fluorescent-labeled DNA probes) to detect chromosomal alterations of malignant cells has been found to be more specific for the detection of malignant strictures compared with routine cytology brushing (98% vs 91%, respectively) however, for most institutions, FISH analysis delays the diagnosis and may not be cost effective [3].
EC is often mistaken for cholangiocarcinoma, leading to unnecessary surgical intervention including, but not limited to, liver resection, cholecystectomy, common bile duct resection, and hepaticojejunostomy or pancreaticoduodenectomy [10]. In our review of the literature, 66% of the cases had surgery, with 52% of those being successfully treated with surgery alone. Currently, 10-24% of all liver resections result in benign biliary pathology [1, 3]. Matsumoto et al, describes diagnostic criteria for EC as 1) wall thickening and stenosis of biliary system on imaging, 2) eosinophilic infiltration on pathology (either biopsy or resection), and 3) reversibility of symptoms with steroids [3,9]. To prevent unnecessary surgical resection, EC should be diagnosed by non-resectional biopsy and since individual case studies of EC have shown the benefit of high-dose steroids (prednisone 60mg daily for 2 weeks and then tapered over 6 months) with biliary stenting as needed for obstructive symptoms, the goal would-be disease-free survival without resection [1, 9]. Unfortunately, the dire consequences of missing a malignant disease cannot be ignored. Thus, many cases fall to surgical resection due to diagnostic uncertainty.
We reviewed 36 case reports of patients who were diagnosed with EC and evaluated the literature along with the two cases reported here. The most common presentation included abdominal pain (23 of 38 patients, 61%), with 55% (12 out of 22 patients) having concomitant jaundice. Jaundice alone at initial presentation was reported in 6 out of 38 patients (16%). Less commonly, patients presented with associated fever (16%) or pruritis (15%). Imaging was discussed in 28 of the 38 case reports and bile duct stenosis was identified in 22 patients (78%), suggesting mass effect (Table 1 and 2). Other abnormalities included unspecified intrahepatic ductal dilation in 6 patients, and biliary dilation alone in 1 patient. Surgical intervention was completed on 25 patients, including wedge biopsy, roux-en Y hepaticojejunostomy, cholecystectomy or pancreaticoduodenectomy. Of these, 12 underwent additional post-surgical management that included corticosteroids, ursodiol, hydroxurea, azathioprine, benzafibrate or mesalazine. Medical management was the only treatment in 11 patients. Of the 38 cases, 31 commented on recurrence of which 21 reported actual follow-up times (2 months to 14 years; Table 1). In the 31 patients in whom recurrence was commented on, 26 (84%) had no recurrence. This group included 9 patients treated with surgery only, 9 patients that had surgery and medical treatment, and 7 patients with medical intervention only. A small subset (5/31; 16%; Table 1) were identified as having recurrent disease.
To date, we have completed the most comprehensive literature review comparing age, race, gender, presenting symptoms, presence of eosinophilic infiltrate and biliary stricture, as well as comparisons of surgery versus medical management with corresponding outcomes (Table 1). This review has prompted the development of a decision algorithm concerning appropriate management of possible EC patients (Figure 5). The conventional demographic profile of an EC patient is middle-aged (< 60) presenting with abdominal pain and jaundice. An evaluation of liver function (LFTs) and imaging should be completed. If LFTs are within normal limits and a mass and/or biliary stricture/dilation is identified, peripheral eosinophilia should be assessed. Presence of peripheral eosinophilia dictates medical management; however, absence of peripheral eosinophilia is suggestive pathologic evaluation through biopsy. Histologic structure and specific staining can differentiate inflammation, eosinophilia and malignancy, suggesting the appropriate treatment for the patient while avoiding unnecessary surgical resections.
Table I. Literature Review (n=38)
|
Author |
Yr |
Age |
Race |
Gender |
Presenting Symptoms |
PRHE |
PREI |
REI |
PE |
Stricture site |
Surgery |
Medical Tx |
Outcomes |
|
Leegaard*4 |
1980 |
46 |
- |
M |
Abdominal pain, jaundice-- |
|
|
Y |
|
CBD |
CE |
CS |
No recurrence at 18 mo |
|
Butler*5 |
1985 |
32 |
B |
M |
Abdominal pain |
|
|
Y |
Y |
CBD |
CE |
- |
No recurrence at 24mo |
|
Rosengart11 |
1990 |
48 |
W |
M |
Abdominal pain, jaundice |
N |
|
Y |
N |
CHD |
CE |
- |
No recurrence at 9 mo |
|
Platt12 |
1990 |
56 |
A |
F |
Jaundice/Utreteric obs |
Y |
E |
Y |
N |
CBD |
CE |
- |
Recurrence 14y as ureteritis |
|
Scheurlen13 |
1992 |
28 |
- |
M |
Abdominal pain, diarrhea |
Y |
E |
Y |
Y |
CBD/IHBD |
- |
Hydroxurea |
No recurrence |
|
Grauer14 |
1993 |
41 |
H |
M |
Abdominal pain, jaundice, fever |
Y |
E |
Y |
Y |
EHBD† |
- |
CS, Ursodiol |
Recurrence in kidney |
|
Schoonbroodt15 |
1995 |
20 |
- |
M |
Jaundice, fever |
Y |
E |
Y |
Y |
IHBD |
CE |
CS |
Recurrence in stomach |
|
Tenner16 |
1997 |
38 |
- |
F |
Abdominal pain |
Y |
I |
Y |
Y |
CBD/IHBD |
CE |
CS |
No recurrence 3mo |
|
Song17 |
1997 |
48 |
- |
F |
Abdominal pain |
Y’ |
NMCP |
Y |
Y |
CBD |
CE, T-tube |
- |
No recurrence at 9mo |
|
Al-Abdulla18 |
2000 |
42 |
- |
F |
Abdominal Pain, jaundice |
N |
|
Y |
Y |
IHBD |
CE |
CS |
|
|
Rodgers8 |
2001 |
50 |
W |
F |
Epigastric pain, Nausea, Vomiting |
Y’ |
I |
Y |
N |
CBD |
Roux-en-Y/CE |
- |
No recurrence at 2 mo |
|
Shanti19 |
2001 |
33 |
B |
M |
Abdominal pain, jaundice |
N |
|
Y |
N |
IHBD (bilat) |
CE, hepatojejunostomy |
- |
No recurrence 3mo |
|
Shanti19 |
2001 |
57 |
B |
F |
Abdominal pain, jaundice |
Y |
I |
Y |
N |
CBD |
Roux-en-Y |
- |
No recurrence 6mo |
|
Vauthey2 |
2003 |
44 |
- |
M |
Abdominal pain, jaundice |
Y |
NMCP |
Y |
Y |
CBD (distal) |
- |
CS |
No recurrence 18mo |
|
Jimenez-Saenz20 |
2003 |
67 |
- |
F |
Abdominal pain, jaundice |
Y |
E |
Y |
Y |
IHBD/EHBD† |
CE |
CS |
No recurrence 12mo |
|
Duseja21 |
2005 |
16 |
- |
F |
Abdominal Pain, jaundice |
Y |
NMECP |
Y |
Y |
CBD |
- |
CS |
No recurrence 12mo |
|
Matsumoto9 |
2007 |
38 |
A |
F |
Abdominal Pain, jaundice |
Y |
E |
Y |
Y |
IHBD |
- |
CS |
No recurrence 5mo |
|
Jeyamani 22 |
2007 |
13 |
- |
M |
Abdominal Pain |
Y |
E |
Y |
Y |
CBD |
- |
CS |
Recurrence in liver |
|
Jeyamani22 |
2007 |
26 |
- |
M |
Fever, pruritis |
Y |
E |
Y |
Y |
CBD/CHD/IHBD |
Biliary sphincterotomy |
CS |
No recurrence 6mo |
|
Sussman23 |
2008 |
52 |
W |
M |
Abdominal pain, pruritis |
Y |
E |
Y |
Y |
Liver sinusoids |
- |
CS, AZT, UDCA |
No recurrence |
|
Horiuchi24 |
2009 |
45 |
A |
M |
Liver dysfunction |
Y |
E |
Y |
Y |
IHBD |
- |
UDCA, Bezafibrate |
|
|
Miura10 |
2009 |
46 |
A |
M |
Jaundice |
N |
|
Y |
N |
IHBD/EHBD† |
Pylorus preserving pancreatoduodenectomy; wedge liver biopsy; |
- |
|
|
Chen25 |
2009 |
55 |
- |
M |
Jaundice |
Y |
NMCP |
Y |
Y |
IHBD (bilat)/CBD/CHD |
Roux-en-Y, CE |
CS |
No recurrence 9mo |
|
Raptou26 |
2009 |
24 |
- |
M |
Abdominal Pain |
N |
|
Y |
Y |
IHBD |
Cyst removal; wedge bx |
Albendazole |
No recurrence |
|
Iwamuro27 |
2009 |
66 |
A |
F |
Jaundice |
Y |
I |
Y |
Y |
IHBD/EHBD† |
- |
CS |
|
|
Nashed3 |
2010 |
33 |
W |
M |
Jaundice, Pruritis, |
Y |
NMCP |
Y |
N |
CHD |
Roux-en-Y/CE, CBD resect, |
- |
No recurrence 40mo |
|
Dubay28 |
2010 |
29 |
W |
F |
Abdominal pain, nausea, pruritis |
Y |
NMCP |
Y |
Y |
CBD |
Roux-en-Y |
- |
|
|
Ling29 |
2011 |
58 |
- |
F |
Abdominal pain, icterus, nausea |
Y |
E |
Y |
Y |
CBD |
- |
- |
Spontaneous remission |
|
Kroemer30 |
2012 |
49 |
- |
M |
Abdominal pain, jaundice |
Y |
I |
Y |
N |
CPD/CBD |
Pancreatoduodenectomy |
- |
|
|
Kimura*31 |
2013 |
48 |
- |
M |
Eosinophilia |
Y |
E |
Y |
Y |
Almost normal liver and BD |
CE |
CS |
|
|
Hokuto32 |
2014 |
73 |
A |
M |
Incidental finding |
Y |
NMCP |
Y |
Y |
CBD |
CE |
CS |
No recurrence |
|
Gunji33 |
2014 |
39 |
A |
M |
Abdominal Pain |
Y |
E |
Y |
Y |
IHBD (bilat)/CBD |
- |
CS, UDCA, mesalazine, benzafibrat |
Multiple recurrences |
|
Seow-En34 |
2014 |
63 |
A |
M |
Epigastric Pain, Jaundice |
Y |
NMCP |
Y |
Y |
CBD/CHD |
open cholecystectomy, excision of supraduodenal CBD, Roux-en-Y hepaticojejunostomy |
CS |
No recurrence 6mo |
|
Vainer35 |
2014 |
15 |
- |
F |
Jaundice |
Y |
E |
Y |
|
IHBD (bilat) |
Laproscopic CE |
CS/azathiprine |
No recurrence 12mo |
|
Fragulidis1 |
2015 |
27 |
W |
F |
Abdominal pain, jaundice |
Y |
I |
Y |
Y |
IHBD |
- |
CS |
No recurrence 18mo |
|
Walter36 |
2017 |
41 |
- |
F |
Abdominal pain, icterus |
Y |
E |
Y |
N |
CBD |
- |
CS |
No recurrence |
|
Krishna |
2017 |
49 |
W |
M |
Abdominal pain |
N |
|
Y |
N |
IHBD |
Left Hepatic Lobectomy |
- |
No recurrence 6mo |
|
Krishna |
2017 |
47 |
W |
F |
Pruritis |
N |
|
Y |
N |
IHBD |
R Hepatic Lobectomy |
- |
No recurrence 5y |
PRHE is the pre-resection histologic evaluation of tissue by biopsy, frozen section, FNA, or brushings; PREI refers to the identification of eosinophilic infiltrate on the pre-resection specimen; REI indicates the state of eosinophilic infiltrate on the resection specimen; PE refers to the identification of eosinophilia in the peripheral blood; *=denotes that the original article was not available or in a language other than English; Greyed boxes indicate that the information was not available.
Eos infiltrate indicates eosinophilic infiltrate on the biopsy or specimen; Abn PE=abnormal peripheral eosinophilia; Stricture site denotes identification on imaging; Stricture location denotations are as follows: CBD=Common Bile Duct, CHD=Common Hepatic Duct, IHBD=Intra-hepatic Bile Duct, †EHBD=Extrahepatic Bile Duct (authors did not differentiate CHD from CBD), CPD=Common Pancreatic Duct; CE = Cholecystectomy; Medical Therapy is denoted as follows: CS = Corticosteroids, AZT = Azathioprine, UDCA = Ursodeoxycholic Acid; grey boxes indicate information was not given.
Table II. Summary of the Literature
|
|
|
|
|
Age |
|
|
|
Mean |
42 |
|
|
Median |
44.5 |
|
|
Range |
13-73 |
|
|
Gender |
|
|
|
Male |
22 (58%) |
|
|
Female |
16 (42%) |
|
|
Race |
|
|
|
White |
8 (21%) |
|
|
Black |
3 (8%) |
|
|
Hispanic |
1 (3%) |
|
|
Asian |
8 (21%) |
|
|
Not reported |
18 (47%) |
|
|
Symptoms |
|
|
|
Abd. pain |
24 (63%) |
|
|
Jaundice |
20 (53%) |
|
|
Other |
13 (34%) |
|
|
Incidental Finding |
1 (3%) |
|
|
PE |
|
|
|
Yes |
25 (66%) |
|
|
No |
11 (29%) |
|
|
Unknown |
2 (5%) |
|
|
Location of Stricture |
|
|
|
CBD |
20 (53%) |
|
|
CHD |
5 (13%) |
|
|
IHBD |
17 (45%) |
|
|
EHBD |
4 (11%) |
|
|
Multiple |
10 (26%) |
|
|
Other |
3 (8%) |
|
|
PRHE (n=36) |
|
|
|
Yes |
29 (77%) |
|
|
Eosinophils |
15 (52%) |
|
|
Surg |
1 (7%) |
|
|
Med |
8 (53%) |
|
|
S+M |
5 (33%) |
|
|
Inflammation |
6 (16%) |
|
|
Surg |
3 (50%) |
|
|
Med |
2 (33%) |
|
|
S+M |
1 (17%) |
|
|
‘no malignant cells’ |
8 (21%) |
|
|
Surg |
3 (38%) |
|
|
Med |
2 (25%) |
|
|
S+M |
3 (38%) |
|
|
No |
7 (18%) |
|
|
Not reported |
2 (5%) |
|
|
REI |
|
|
|
Yes |
38 (100%) |
|
|
No |
0 |
|
|
Treatment |
|
|
|
Surgery |
25 (66%) |
|
|
Surg only |
13 (52%) |
|
|
Medical |
24 (63%) |
87.5% CS* |
|
Med Only |
12 (50%) |
|
|
Surg + Med |
12 (32%) |
|
|
No tx |
1 (3%) |
|
|
Outcomes |
|
|
|
Recurrence |
5 (13%) |
|
|
Surg |
1 (20%) |
|
|
Med |
3 (60%) |
|
|
Both |
1 (20%) |
|
|
No Recurrence |
25 (66%) |
|
|
Surg |
9 (36%) |
|
|
Med |
7 (28%) |
|
|
Both |
9 (36%) |
|
|
†Spontaneous |
1 (3%) |
|
|
Not reported |
7 (18%) |
|
PRHE=pre-resection histologic evaluation; REI=resection eosinophilic infiltrate; PE=peripheral
Eosinophilia; *the primary medical treatment was reported to be corticosteroids;
†case report indicated no surgical or medical management of the patient and the case was
reported as a spontaneous remission
Conclusion
Eosinophilic Cholangitis is a rare, benign biliary pathology often mistaken for cholangiocarcinoma, leading to extensive surgical resections and increased morbidity and mortality. Therefore, it is important to keep EC in addition to other benign biliary diseases in mind when working up obstructive biliary disease.
Disclosures
The authors report that there is nothing to disclose.
Article Info
Article Type
Case Report and Review of the LiteratureArticle History
Received 9 October , 2018Accepted 30 October , 2018
Published 14 November, 2018
Copyright
© 2018 The Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.10.31487/j.SCR.2018.03.013
Author Info
Corresponding author
Steven D Trocha MD890 W Faris Rd Suite 320, Greenville, SC 29605.
Figures & Tables
Table I. Literature Review (n=38)
|
Author |
Yr |
Age |
Race |
Gender |
Presenting Symptoms |
PRHE |
PREI |
REI |
PE |
Stricture site |
Surgery |
Medical Tx |
Outcomes |
|
Leegaard*4 |
1980 |
46 |
- |
M |
Abdominal pain, jaundice-- |
|
|
Y |
|
CBD |
CE |
CS |
No recurrence at 18 mo |
|
Butler*5 |
1985 |
32 |
B |
M |
Abdominal pain |
|
|
Y |
Y |
CBD |
CE |
- |
No recurrence at 24mo |
|
Rosengart11 |
1990 |
48 |
W |
M |
Abdominal pain, jaundice |
N |
|
Y |
N |
CHD |
CE |
- |
No recurrence at 9 mo |
|
Platt12 |
1990 |
56 |
A |
F |
Jaundice/Utreteric obs |
Y |
E |
Y |
N |
CBD |
CE |
- |
Recurrence 14y as ureteritis |
|
Scheurlen13 |
1992 |
28 |
- |
M |
Abdominal pain, diarrhea |
Y |
E |
Y |
Y |
CBD/IHBD |
- |
Hydroxurea |
No recurrence |
|
Grauer14 |
1993 |
41 |
H |
M |
Abdominal pain, jaundice, fever |
Y |
E |
Y |
Y |
EHBD† |
- |
CS, Ursodiol |
Recurrence in kidney |
|
Schoonbroodt15 |
1995 |
20 |
- |
M |
Jaundice, fever |
Y |
E |
Y |
Y |
IHBD |
CE |
CS |
Recurrence in stomach |
|
Tenner16 |
1997 |
38 |
- |
F |
Abdominal pain |
Y |
I |
Y |
Y |
CBD/IHBD |
CE |
CS |
No recurrence 3mo |
|
Song17 |
1997 |
48 |
- |
F |
Abdominal pain |
Y’ |
NMCP |
Y |
Y |
CBD |
CE, T-tube |
- |
No recurrence at 9mo |
|
Al-Abdulla18 |
2000 |
42 |
- |
F |
Abdominal Pain, jaundice |
N |
|
Y |
Y |
IHBD |
CE |
CS |
|
|
Rodgers8 |
2001 |
50 |
W |
F |
Epigastric pain, Nausea, Vomiting |
Y’ |
I |
Y |
N |
CBD |
Roux-en-Y/CE |
- |
No recurrence at 2 mo |
|
Shanti19 |
2001 |
33 |
B |
M |
Abdominal pain, jaundice |
N |
|
Y |
N |
IHBD (bilat) |
CE, hepatojejunostomy |
- |
No recurrence 3mo |
|
Shanti19 |
2001 |
57 |
B |
F |
Abdominal pain, jaundice |
Y |
I |
Y |
N |
CBD |
Roux-en-Y |
- |
No recurrence 6mo |
|
Vauthey2 |
2003 |
44 |
- |
M |
Abdominal pain, jaundice |
Y |
NMCP |
Y |
Y |
CBD (distal) |
- |
CS |
No recurrence 18mo |
|
Jimenez-Saenz20 |
2003 |
67 |
- |
F |
Abdominal pain, jaundice |
Y |
E |
Y |
Y |
IHBD/EHBD† |
CE |
CS |
No recurrence 12mo |
|
Duseja21 |
2005 |
16 |
- |
F |
Abdominal Pain, jaundice |
Y |
NMECP |
Y |
Y |
CBD |
- |
CS |
No recurrence 12mo |
|
Matsumoto9 |
2007 |
38 |
A |
F |
Abdominal Pain, jaundice |
Y |
E |
Y |
Y |
IHBD |
- |
CS |
No recurrence 5mo |
|
Jeyamani 22 |
2007 |
13 |
- |
M |
Abdominal Pain |
Y |
E |
Y |
Y |
CBD |
- |
CS |
Recurrence in liver |
|
Jeyamani22 |
2007 |
26 |
- |
M |
Fever, pruritis |
Y |
E |
Y |
Y |
CBD/CHD/IHBD |
Biliary sphincterotomy |
CS |
No recurrence 6mo |
|
Sussman23 |
2008 |
52 |
W |
M |
Abdominal pain, pruritis |
Y |
E |
Y |
Y |
Liver sinusoids |
- |
CS, AZT, UDCA |
No recurrence |
|
Horiuchi24 |
2009 |
45 |
A |
M |
Liver dysfunction |
Y |
E |
Y |
Y |
IHBD |
- |
UDCA, Bezafibrate |
|
|
Miura10 |
2009 |
46 |
A |
M |
Jaundice |
N |
|
Y |
N |
IHBD/EHBD† |
Pylorus preserving pancreatoduodenectomy; wedge liver biopsy; |
- |
|
|
Chen25 |
2009 |
55 |
- |
M |
Jaundice |
Y |
NMCP |
Y |
Y |
IHBD (bilat)/CBD/CHD |
Roux-en-Y, CE |
CS |
No recurrence 9mo |
|
Raptou26 |
2009 |
24 |
- |
M |
Abdominal Pain |
N |
|
Y |
Y |
IHBD |
Cyst removal; wedge bx |
Albendazole |
No recurrence |
|
Iwamuro27 |
2009 |
66 |
A |
F |
Jaundice |
Y |
I |
Y |
Y |
IHBD/EHBD† |
- |
CS |
|
|
Nashed3 |
2010 |
33 |
W |
M |
Jaundice, Pruritis, |
Y |
NMCP |
Y |
N |
CHD |
Roux-en-Y/CE, CBD resect, |
- |
No recurrence 40mo |
|
Dubay28 |
2010 |
29 |
W |
F |
Abdominal pain, nausea, pruritis |
Y |
NMCP |
Y |
Y |
CBD |
Roux-en-Y |
- |
|
|
Ling29 |
2011 |
58 |
- |
F |
Abdominal pain, icterus, nausea |
Y |
E |
Y |
Y |
CBD |
- |
- |
Spontaneous remission |
|
Kroemer30 |
2012 |
49 |
- |
M |
Abdominal pain, jaundice |
Y |
I |
Y |
N |
CPD/CBD |
Pancreatoduodenectomy |
- |
|
|
Kimura*31 |
2013 |
48 |
- |
M |
Eosinophilia |
Y |
E |
Y |
Y |
Almost normal liver and BD |
CE |
CS |
|
|
Hokuto32 |
2014 |
73 |
A |
M |
Incidental finding |
Y |
NMCP |
Y |
Y |
CBD |
CE |
CS |
No recurrence |
|
Gunji33 |
2014 |
39 |
A |
M |
Abdominal Pain |
Y |
E |
Y |
Y |
IHBD (bilat)/CBD |
- |
CS, UDCA, mesalazine, benzafibrat |
Multiple recurrences |
|
Seow-En34 |
2014 |
63 |
A |
M |
Epigastric Pain, Jaundice |
Y |
NMCP |
Y |
Y |
CBD/CHD |
open cholecystectomy, excision of supraduodenal CBD, Roux-en-Y hepaticojejunostomy |
CS |
No recurrence 6mo |
|
Vainer35 |
2014 |
15 |
- |
F |
Jaundice |
Y |
E |
Y |
|
IHBD (bilat) |
Laproscopic CE |
CS/azathiprine |
No recurrence 12mo |
|
Fragulidis1 |
2015 |
27 |
W |
F |
Abdominal pain, jaundice |
Y |
I |
Y |
Y |
IHBD |
- |
CS |
No recurrence 18mo |
|
Walter36 |
2017 |
41 |
- |
F |
Abdominal pain, icterus |
Y |
E |
Y |
N |
CBD |
- |
CS |
No recurrence |
|
Krishna |
2017 |
49 |
W |
M |
Abdominal pain |
N |
|
Y |
N |
IHBD |
Left Hepatic Lobectomy |
- |
No recurrence 6mo |
|
Krishna |
2017 |
47 |
W |
F |
Pruritis |
N |
|
Y |
N |
IHBD |
R Hepatic Lobectomy |
- |
No recurrence 5y |
PRHE is the pre-resection histologic evaluation of tissue by biopsy, frozen section, FNA, or brushings; PREI refers to the identification of eosinophilic infiltrate on the pre-resection specimen; REI indicates the state of eosinophilic infiltrate on the resection specimen; PE refers to the identification of eosinophilia in the peripheral blood; *=denotes that the original article was not available or in a language other than English; Greyed boxes indicate that the information was not available.
Eos infiltrate indicates eosinophilic infiltrate on the biopsy or specimen; Abn PE=abnormal peripheral eosinophilia; Stricture site denotes identification on imaging; Stricture location denotations are as follows: CBD=Common Bile Duct, CHD=Common Hepatic Duct, IHBD=Intra-hepatic Bile Duct, †EHBD=Extrahepatic Bile Duct (authors did not differentiate CHD from CBD), CPD=Common Pancreatic Duct; CE = Cholecystectomy; Medical Therapy is denoted as follows: CS = Corticosteroids, AZT = Azathioprine, UDCA = Ursodeoxycholic Acid; grey boxes indicate information was not given.
Table II. Summary of the Literature
|
|
|
|
|
Age |
|
|
|
Mean |
42 |
|
|
Median |
44.5 |
|
|
Range |
13-73 |
|
|
Gender |
|
|
|
Male |
22 (58%) |
|
|
Female |
16 (42%) |
|
|
Race |
|
|
|
White |
8 (21%) |
|
|
Black |
3 (8%) |
|
|
Hispanic |
1 (3%) |
|
|
Asian |
8 (21%) |
|
|
Not reported |
18 (47%) |
|
|
Symptoms |
|
|
|
Abd. pain |
24 (63%) |
|
|
Jaundice |
20 (53%) |
|
|
Other |
13 (34%) |
|
|
Incidental Finding |
1 (3%) |
|
|
PE |
|
|
|
Yes |
25 (66%) |
|
|
No |
11 (29%) |
|
|
Unknown |
2 (5%) |
|
|
Location of Stricture |
|
|
|
CBD |
20 (53%) |
|
|
CHD |
5 (13%) |
|
|
IHBD |
17 (45%) |
|
|
EHBD |
4 (11%) |
|
|
Multiple |
10 (26%) |
|
|
Other |
3 (8%) |
|
|
PRHE (n=36) |
|
|
|
Yes |
29 (77%) |
|
|
Eosinophils |
15 (52%) |
|
|
Surg |
1 (7%) |
|
|
Med |
8 (53%) |
|
|
S+M |
5 (33%) |
|
|
Inflammation |
6 (16%) |
|
|
Surg |
3 (50%) |
|
|
Med |
2 (33%) |
|
|
S+M |
1 (17%) |
|
|
‘no malignant cells’ |
8 (21%) |
|
|
Surg |
3 (38%) |
|
|
Med |
2 (25%) |
|
|
S+M |
3 (38%) |
|
|
No |
7 (18%) |
|
|
Not reported |
2 (5%) |
|
|
REI |
|
|
|
Yes |
38 (100%) |
|
|
No |
0 |
|
|
Treatment |
|
|
|
Surgery |
25 (66%) |
|
|
Surg only |
13 (52%) |
|
|
Medical |
24 (63%) |
87.5% CS* |
|
Med Only |
12 (50%) |
|
|
Surg + Med |
12 (32%) |
|
|
No tx |
1 (3%) |
|
|
Outcomes |
|
|
|
Recurrence |
5 (13%) |
|
|
Surg |
1 (20%) |
|
|
Med |
3 (60%) |
|
|
Both |
1 (20%) |
|
|
No Recurrence |
25 (66%) |
|
|
Surg |
9 (36%) |
|
|
Med |
7 (28%) |
|
|
Both |
9 (36%) |
|
|
†Spontaneous |
1 (3%) |
|
|
Not reported |
7 (18%) |
|
PRHE=pre-resection histologic evaluation; REI=resection eosinophilic infiltrate; PE=peripheral
Eosinophilia; *the primary medical treatment was reported to be corticosteroids;
†case report indicated no surgical or medical management of the patient and the case was
reported as a spontaneous remission
References
1. Fragulidis GP, Vezakis AI, Kontis EA, Pantiora EV, Stefanidis GG, et al. (2016) Eosinophilic Cholangitis--A Challenging Diagnosis of Benign Biliary Stricture: A Case Report. Medicine (Baltimore). [Crossref]
2. Jean-Nicolas Vauthey, Evelyne Loyer, Parag Chokshi, Sandeep Lahoti (2003) Case 57: Eosinophilic Cholangiopathy. Radiology.
3. Nashed C, Sakpal SV, Shusharina V, Chamberlain RS (2010) Eosinophilic Cholangitis and Cholangiopathy: A Sheep in Wolves Clothing. HPB Surgery.
4. Leegaard M (1980) Eosinophilic Cholangitis. Acta Chir Scand 146: 295-296.
5. Butler TW, Feintuch TA, Caine WP Jr (1985) Eosinophilic cholangitis, lymphadenopathy, and peripheral eosinophilia: a case report. Am J Gastroenterol 80: 572–574. [Crossref]
6. Wong DT, Elovic A, Matossian K, Nagura N, McBride J, et al. (1991) Eosinophils from patients with blood eosinophilia express transforming growth factor beta 1. Blood 78: 2702–2707. [Crossref]
7. Baskan O, Erol C, Sahingoz Y (2016) Portal Biliopathy, Magnetic Resonance Imaging and Magnetic Resonance Cholangiopancreaticography findings: a case series. Gastroenterolgoy Rep (Oxf) 4: 68-72. [Crossref]
8. Rodgers MS, Allen JP, Koea JB, McCall JL (2001) Eosinophilic Cholangitis: a case of ‘malignant masquerade’. HPB (Oxford) 3: 235-239. [Crossref]
9. Matsumoto N, Yokoyama K, Nakai K, Yamamoto T, Otani T, et al. (2007) A Case of Eosinophilic Cholangitis: Imaging Findings of Contrast-Enhanced Ultrasonography, Cholangioscopy, and Intraductal Ultrasonography. World J Gastroenterol 13: 1995–1997. [Crossref]
10. Miura F, Asano T, Amano H, Yoshida M, Toyota N, et al. (2009) Resected Case of Eosinophilic Cholangiopathy Presenting with Secondary Sclerosing Cholangitis. World J Gastroenterol 15: 1394–1397. [Crossref]
11. Rosengart TK, Rotterdam H, Ranson JH (1990) Eosinophilic cholangitis: a self-limited cause of extrahepatic biliary obstruction. Am J Gastroenterol 85: 582–585. [Crossref]
12. Platt ML, Kiesling VJ, Vaccaro JA (1990) Eosinophilic ureteritis associated with eosinophilic cholangitis: a case report. J Urol 144: 127–129. [Crossref]
13. Scheurlen M, Mork H, Weber P (1992) Hypereosinophilic syndrome resembling chronic inflammatory bowel disease with primary sclerosing cholangitis. J Clin Gastroenterol 14: 59–63. [Crossref]
14. Grauer L, Padilla VMD, Bouza L, Barkin JS (1993) Eosinophilic sclerosing cholangitis associated with hypereosinophilic syndrome. Am J Gastroenterol 88: 1764–1769. [Crossref]
15. Schoonbroodt D, Horsmans Y, Laka A, Geubel AP, et al. (1995) Eosinophilic cholangiopathy presenting with colitis and cholangitis. Dig Dis Sci 40: 308-314.
16. Tenner S, Roston A, Lichtenstein D, Brooks D, Herlihy E, et al. (1997) Eosinophilic Cholangiopathy. Gastrointest Endosc 45: 307–309. [Crossref]
17. Song H, Byun J, Jung S, Choi KH, Shinn KS, et al. (1997) Eosinophilic cholangitis: US, CT, and cholangiography findings. J Comput Assist Tomogr 21: 251-253. [Crossref]
18. Al-Abdulla NA, Schulick RD, Regan F (2000) Hypereosinophilic sclerosing cholangitis: findings using half-Fourier magnetic resonance imaging. Hepatogastroenterology 47: 359-361. [Crossref]
19. Shanti CM, Lucas CE, Tyburski JG, Soulen RL, Lucas DR, et al. (2001) Eosinophilic abscess and eosinophilic pseudotumor presenting as bile duct masses: a report of 2 cases. Surgery 130: 104-108. [Crossref]
20. Jimenez-Saenz M, Villar-Rodriguez JL, Torres Y, Carmona I, Salas-Herrero E, et al. Biliary tract disease: a rare manifestation of eosinophilic gastroenteritis. Dig Dis Sci 48: 624-627. [Crossref]
21. Duseja, A, Nada R, Dhiman RK, Chawla YK, Kalra N, et al. (2005) Eosinophilic cholangiopathy-a case report. Dig Dis Sci 50: 1422-1425. [Crossref]
22. Jeyamani R, Ramakrishna BS, Kurian G (2007) Eosinophilic cholangiopathy—a report of two cases. Indian J Gastroenterol 26: 190-191. [Crossref]
23. Sussman DA, Bejarano PA, Regev A (2008) Eosinophilic cholangiopathy with concurrent eosinophilic colitis in a patient with idiopathic hypereosinophilic syndrome. Eur J Gastroenterol Hepatol 20: 574-577. [Crossref]
24. Horiuchi K, Kakizaki S, Kosone T, Ichikawa T, Sato K, et al. (2009) Marked eosinophilia as the first manifestation of sclerosing cholangitis. Intern Med 48: 1377-1382. [Crossref]
25. Chen WH, Yu CC, Wu CC, Jan YJ (2009) Eosinophilic cholangitis with obstructive jaundice mimicking bile duct carcinoma. J Hepatobiliary Pancreat Surg 16: 242-245. [Crossref]
26. Raptou G1, Pliakos I, Hytiroglou P, Papavramidis S, Karkavelas G (2009) Severe eosinophilic cholangitis with parenchymal destruction of the left hepatic lobe due to hydatid disease. Pathol Int 59: 395-398. [Crossref]
27. Iwamuro M, Yamamoto K, Kawamoto H, Terada R, Ogawa T, et al. (2009) Eosinophilic cholangitis with initial clinical features indistinguishable from IgG4-related cholangitis. Intern Med 48 :1143-1147. [Crossref]
28. Dubay D, Jhala N, Eloubeidi M (2010) Eosinophilic cholangitis. Clin Gastroenterol Hepatol 8: A22. [Crossref]
29. Ling M, Begun J, Patil S, Hamilos DL (2011) Eosinophilic Cholangiopathy Presenting with Peripheral Eosinophilia and Hepatic Mass. J Allergy Clin Immun 127: 108-108.
30. Kroemer A, Sabet-Baktach M, Doenecke A, Ruemmele P, Scherer MN, et al. (2012) Eosinophilic Cholangitis and Wirsungitis as Cause of Simultaneous Bile Duct Obstruction and Pancreatitis. Z Gastroenterol 50: 766-770. [Crossref]
31. Kimura Y, Yamashita Y, Mikami S, Ono H, Itai R, et al. (2013) Eosinophilic cholangitis from almost normal appearance to the bile duct sclerosis similar to primary sclerosing cholangitis. Nihon Shokakibyo Gakkai Zasshi 110: 271-281. [Crossref]
32. Hokuto D, Yamato I, Nomi T, Yasuda S, Obara S, et al. (2015) Eosinophilic cholangitis coexisted with idiopathic thrombocytopenic purpura: Report of a case. Hepatology Research 45: 595-600. [Crossref]
33. Gunji N, Katakura K, Takahashi A, Fujiwara T, Suzuki R, et al. (2014) Concurrent Primary Sclerosing Cholangitisand Eosinophilic Colitis. Intern Med 53: 2319-2324. [Crossref]
34. Seow-En I, Chiow AK, Tan SS, Poh WT (2014) Eosinophilic Cholangiopathy: The Diagnostic Dilemma of a Recurrent Biliary Stricture. Should Surgery Be Offered for All? BMJ Case Reports. [Crossref]
35. Vainer E, Vainer G, Jacob H, Faroja M (2014) Eosinophilic cholangitis diagnosed endoscopically. Endoscopy 46: 95-96.
36. Walter D, Hartmann S, Herrmann E, Peveling-Oberhag J, et al. (2017) Eosinophilic cholangitis is a potentially underdiagnosed etiology in indeterminate biliary stricture. World J Gastroenterol 23: 1044-1050. [Crossref]