Traumatic Fractures Involving Major Dural Venous Sinuses: A Reappraisal Study from the Tertiary Trauma Care Center in Nepal
A B S T R A C T
Objective: The surgical management of compound depressed fractures overlying dural venous sinuses confers major challenges for the neurosurgeons. On one hand, the depressed fracture and associated compound wound herald the risk of venous occlusion and fatal brain swelling, on the other hand, the surgical attempt in managing them foresees major risks of bleeding and air embolism.
Materials and Results: A retrospective analytical study was conducted from the hospital records pertaining to the cohorts of patients admitted with traumatic fractures overlying major dural venous sinuses. Among 45 patients included on our study, six patients were managed conservatively, and the rest 39 patients required surgical intervention due to compound depressed fractures heralding high risk of venous flow obstruction. The age of our patients ranged from 6 to 60 years with a high male predominance (77% vs. 22.22%).The most common mode of injuries was road traffic accidents in 66.67% (30/45) of cases. The most common location of depressed fracture was in the anterior third of SSS, seen in 57.77% of cases. The surgical complications were seen is 2.23% of cases, with the single instances of air embolism, profuse bleeding and cortical venous thrombosis seen respectively. The overall mortality seen in our study was 6.67%, whereas the operative mortality was only 4.45%.
Conclusion: The refinement in the surgical nuances has now enabled us in managing depressed fractures overlying major dural venous sinuses with minimal risks of complications, thereby preventing the high risks of venous hypertension they otherwise invariably harbinger.
Keywords
Fracture, venous sinuses, management, outcome
Introduction
The management algorithm of compound depressed fractures overlying major dural venous sinuses still remaining debatable issues, mirroring as a double-edged sword. The impingement secondary to the depressed fracture harbingers the risk of venous obstruction leading to intracranial hypertension. Paradoxically, any surgical attempt in managing them lurk high risks of profuse sinus bleeding, high odds of air embolism, and cortical venous thrombosis with haemorrhagic transformation. The incidence of such challenging entity in the current literature is estimated at around 4% [1-4]. The corresponding mortality, in sharp contrast, is seen in as high as 40% of such subsets of patients [5]. There is paucity, in our context, with regards to the patterns of clinical presentation and the outcome analysis pertaining to such important subsets of neurotraumatology. Herein, we attempt to audit the patient demographics, clinical presentations, patterns of management and the final outcome among patients, presenting with compound depressed fracture over dural venous sinuses, in our tertiary care trauma center.
Materials and Methods
A retrospective analytical study was conducted from the hospital records pertaining to the cohorts of patients admitted in the department of Neurosurgery, College of Medical Sciences, Chitwan, Nepal from January 2018 to January 2020 with the diagnosis of traumatic fractures overlying major dural venous sinuses. We reviewed variables pertaining to specific study variables such as demography data, mode of injury, nature of the fractures (linear vs. depressed), presenting Glasgow coma scale, associated intracranial lesions and other specific associate polytrauma, management modalities (conservative vs. surgery), specific complications relating to the injury and the associated mortality. All patients underwent 3D CT imaging reconstruction of the brain to properly categorize the patterns of fractures (Figures 1 & 2).
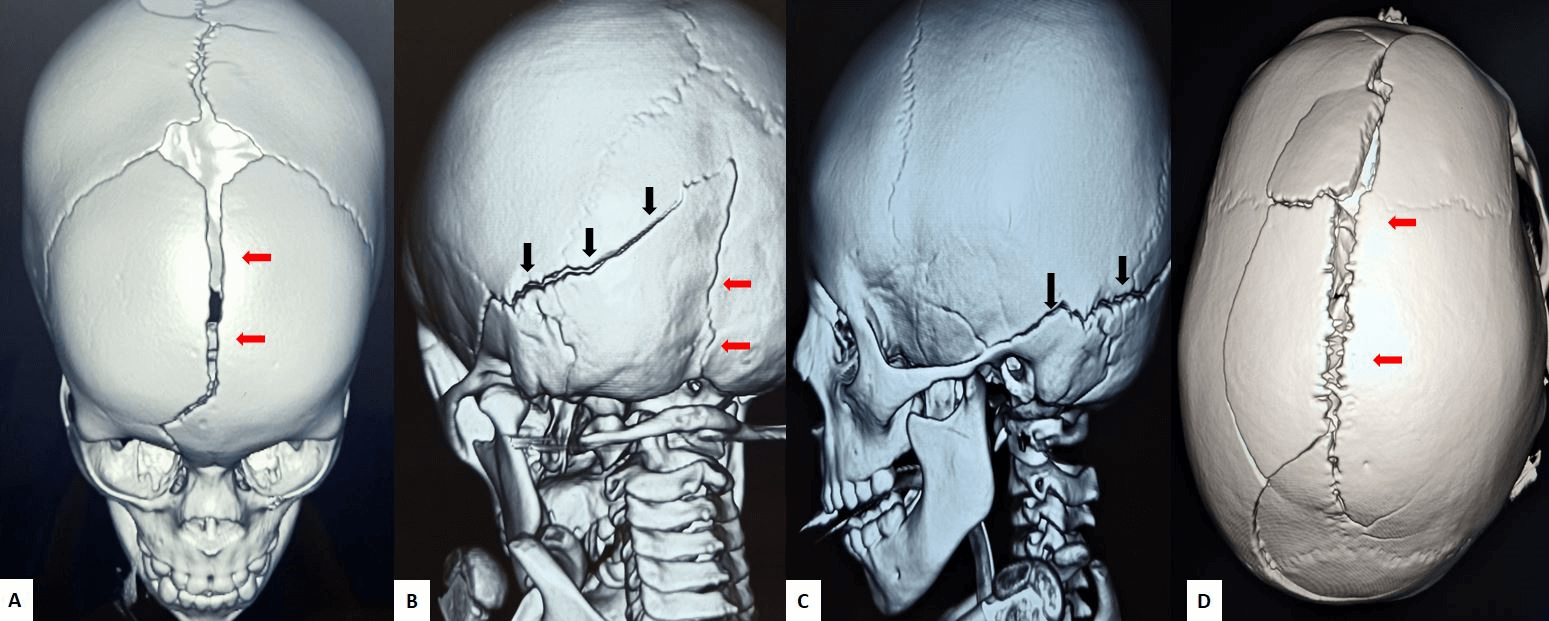
Figure 1: Fractures involving A) anterior sagittal sinus, B) transverse (black arrows) and occipital sinus (red arrows), C) transverse sigmoid sinus junctions and D) middle and posterior superior sagittal sinus.
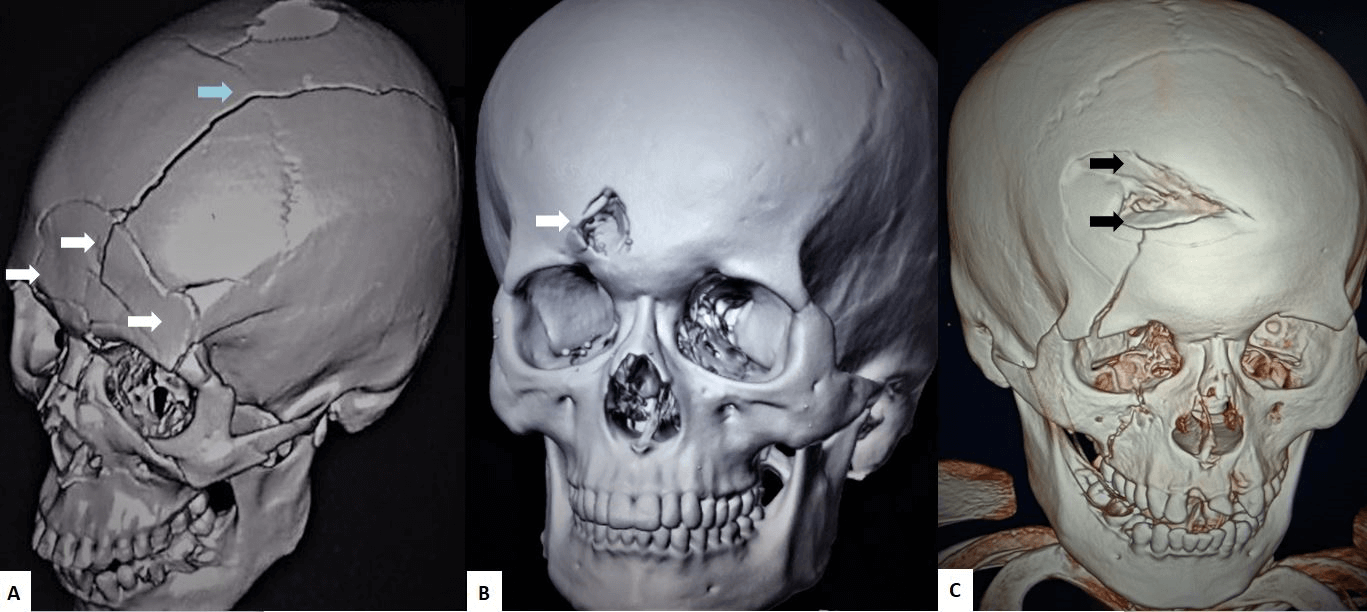
Figure 2: Images depicting A) comminuted fracture involving the anterior superior sagittal sinus and extending to the coronal suture, B) punctate depressed fracture, and C) depressed fractures crossing the anterior third of the superior sagittal sinus.
In case of depressed fracture overlying sinuses, MR venography of the venous sinuses was studied to assess the patency of their patency and also to formulate plan of surgical management. In cases of depressed fractures with normal flow within the sinus and minimal impingements, conservative management was taken. In patient with compromised flow in the dural sinuses along with contaminated compound fractures, operative management was opted. The depressed bone overlying the sinus was elevated and the bony edges near the margins of the sinus were clear fully bitten off with kerrison rongeur. The bleeding was controlled with compression over hemostatic agents such as oxidized regenerated cellulose (surgical) and absorbable gelatin (gel foam) along with continuous saline irrigation over the wound to prevent air embolism. In cases with occasional profuse bleeding, the muscle patch was applied over the sinus and pressure applied. Sometimes the compression was facilitated with the help of continuous dural hitch stiches over the bony bridge placed at the lateral margins of the sinuses. Occasionally, selective coagulation of the bleeding venous channels was carried out. Uncontrollable bleeding in the anterior superior sinus was sometimes controlled by suture ligation. No instances for venous repair were required in our study within the superior sagittal sinus. The fracture segment overlying the middle and the posterior superior sagittal sinus underwent drilling of the overlying bone to eggshell thickness, to prevent the compression as well as prevent bleeding and damages to the draining venous channels. We preserved all the medical related information and autonomy of all of patients in our cohort study. The frequency tabulation and analysis of the results was made with the application of Microsoft Excel software.
Results
Among 45 patients included on our study, six patients were managed conservatively, and the rest 39 patients required surgical intervention due to compound depressed fractures heralding high risk of venous flow obstruction. The age of our patients ranged from 6 to 60 years with a high male predominance (77% vs. 22.22%). In our study, most common mode of injuries accounting to compound depressed fractures underlying dural sinus was road traffic accidents in 66.67% (30/45) of cases. The most common location of depressed fracture over dural venous sinuses seen was in the anterior third of SSS, seen in 57.77% of cases (26/45 cases). The concurrent intracranial lesions associated with the fractures included extradural hematoma (EDH) and pneumocephalus in 37.77% and 22.22% of cases, respectively.
Among the cases that were managed surgically, complications were seen is 2.23% of cases, with the single instances of air embolism, profuse bleeding and cortical venous thrombosis seen respectively. The overall mortality seen in our study was 3 (6.67%), whereas the operative mortality was only 4.45% (2 out of 45). The results in our study have been tabulated and summarized in (Table 1).
Table 1: Demographic and clinical profile of patients with fractures over the dural venous sinus.
|
Variable |
Frequency |
Percentage |
|
Age |
|
|
|
< 10 |
3 |
6.66 |
|
10 -40 |
31 |
68.88 |
|
41 -60 |
11 |
24.44 |
|
Gender |
|
|
|
Male |
35 |
77.77 |
|
female |
10 |
22.22 |
|
Mode of injury |
|
|
|
RTA |
30 |
66.66 |
|
Fall injury |
14 |
31.1 |
|
Physical assault |
1 |
2.22 |
|
Level of consciousness (GCS) |
|
|
|
Mild :13-15 |
29 |
64.44 |
|
Moderate: 9-12 |
9 |
20 |
|
Severe : 3-8 |
7 |
15.5 |
|
Localization of CDF |
|
|
|
Anterior |
26 |
57.77 |
|
Middle |
11 |
24.44 |
|
Posterior |
3 |
6.66 |
|
Transverse sinus |
8 |
17.77 |
|
Associated injuries |
|
|
|
EDH |
17 |
37.77 |
|
SDH |
4 |
8.88 |
|
Contusion |
8 |
17.77 |
|
SAH |
3 |
6.66 |
|
Dural tear |
8 |
17.77 |
|
Pneumocephalus |
10 |
22.22 |
|
Maxillofacial and long bone fracture |
16 |
35.55 |
CDF: Compound Depressed Fracture; GCS: Glasgow Coma Scale; EDH: Extradural Hematoma; SDH: Subdural Hematoma; SAH: Subarachnoid Haemorrhage.
Discussion
The surgical management of compound depressed fractures overlying dural venous sinuses confers major challenges for the neurosurgeons. On one hand, the depressed fracture and associated compound wound herald the risk of venous occlusion and fatal brain swelling, on the other hand, the surgical attempt in managing them foresees major risks of bleeding and air embolism [6, 7]. With regards the mode of injury, road traffic accident (RTA) accounted in almost 80% of cases in a study by Ahmad et al. [8]. However, a study by Aziz et al. showed direct coup injury amounted for most of their patients (58.8%) [9]. In our study, RTA was the main cause of injury (66.67%). The involvement of the anterior third of the superior sagittal sinus (SSS) was seen in almost 70-80% of cases [8-11]. In our study as well, 57.77% patients were involved of anterior superior sagittal sinus.
The need for the surgical management was seen in 52.9% cases in the study by Aziz et al. whereas in our study, 86.67% were treated surgically and only 13.33% were managed with conservative measures [9]. Ours being the tertiary referral center, we mostly do teleconference with the peripheral hospitals regarding the pattern of injuries in the patient and only needful patients in utmost need of surgical management are triaged for the referrals to our center. In the study by Ahmad et al. study, neurological deficits and wound infections were in 4.4% of cases each with the overall mortality of 5.6% [8]. In another study by Elkatatny et al., among eight cases with complications, 62.5% had profuse bleeding [10]. In our study, only three cases had complications, among which one (2.23%) had severe bleeding, followed by air embolism in 2.23% and cortical venous thrombosis in 2.23% of cases, respectively.
In the study of Kim et al., the overall mortality was seen among 15% of cases, consistent with the similar finding seen in the study by Meirowsky et al. [11, 12]. The overall mortality rate in this study was found to be 6.67%. The major cause for the mortality was profuse bleeding and air embolism, however the refinement and advances in the surgical nuances in management have helped in sharp decline in the mortality from previously reported 80% to mere 12% [12, 13]. The eggshell drilling of the depressed segment helps in bony decompression obviating the major risk of bleeding [14]. Another controversial aspect in the management of such lesions is the role of anticoagulants in minimizing the risk of venous thrombosis. However, studies have verified spontaneous recanalization of the venous channels [15]. It also mitigates the risk of intraoperative bleeding that may be required in subsets of these specific patients [15]. In current perspectives, the risk of neurological deficits from not operating on these patients far outweigh the previously feared operative concerns in these cohorts of patients [14].
Conclusion
The refinement in the surgical nuances has now enabled us in managing depressed fractures overlying major dural venous sinuses with minimal risks of complications, thereby preventing the high risks of venous hypertension they otherwise invariably harbinger.
Competing Interest
None.
Funding
None.
Article Info
Article Type
Research ArticlePublication history
Received: Tue 19, May 2020Accepted: Fri 12, Jun 2020
Published: Tue 30, Jun 2020
Copyright
© 2023 Sunil Munakomi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JBN.2020.01.04
Figures & Tables
Table 1: Demographic and clinical profile of patients with fractures over the dural venous sinus.
|
Variable |
Frequency |
Percentage |
|
Age |
|
|
|
< 10 |
3 |
6.66 |
|
10 -40 |
31 |
68.88 |
|
41 -60 |
11 |
24.44 |
|
Gender |
|
|
|
Male |
35 |
77.77 |
|
female |
10 |
22.22 |
|
Mode of injury |
|
|
|
RTA |
30 |
66.66 |
|
Fall injury |
14 |
31.1 |
|
Physical assault |
1 |
2.22 |
|
Level of consciousness (GCS) |
|
|
|
Mild :13-15 |
29 |
64.44 |
|
Moderate: 9-12 |
9 |
20 |
|
Severe : 3-8 |
7 |
15.5 |
|
Localization of CDF |
|
|
|
Anterior |
26 |
57.77 |
|
Middle |
11 |
24.44 |
|
Posterior |
3 |
6.66 |
|
Transverse sinus |
8 |
17.77 |
|
Associated injuries |
|
|
|
EDH |
17 |
37.77 |
|
SDH |
4 |
8.88 |
|
Contusion |
8 |
17.77 |
|
SAH |
3 |
6.66 |
|
Dural tear |
8 |
17.77 |
|
Pneumocephalus |
10 |
22.22 |
|
Maxillofacial and long bone fracture |
16 |
35.55 |
CDF: Compound Depressed Fracture; GCS: Glasgow Coma Scale; EDH: Extradural Hematoma; SDH: Subdural Hematoma; SAH: Subarachnoid Haemorrhage.
References
- Rivkin MA, Saraiya PV, Woodrow SI (2014) Sinovenous thrombosis associated with skull fracture in the setting of blunt head trauma. Acta Neurochir (Wien) 156: 999-1007. [Crossref]
- Kapp JP, Gielchinsky I (1972) Management of combat wounds of the dural venous sinuses. Surgery 71: 913- 917. [Crossref]
- Kapp JP, GIelchinsky I, Deardourff SL (1977) Operative techniques for management of lesions involving the dural venous sinuses. Surg Neurol 7: 339-342. [Crossref]
- Rish BL (1971) The repair of dural venous sinus wounds by autogenous venorrhaphy. J Neurosurg 35: 392-395. [Crossref]
- Meier U, Gartner F, Knopf W, Klötzer R, Wolf O (1992) The traumatic dural sinus injury a clinical study. Acta Neurochir (Wien) 119: 91-93. [Crossref]
- Tanaka H, Tanaka H, Kobata H (2004) Superior sagittal sinus occlusion caused by a compound depressed skull fracture: A case treated by emergency surgery. No Shinkei Geka 32: 753-758. [Crossref]
- Sheng HS, Shen F, Lin J, Bai G, Lin F et al. (2017) Traumatic open depressed cranial fracture causing occlusion of posterior superior sagittal sinus: Case report. Medicine (Baltimore) 96 : e7055. [Crossref]
- Ahmad S, Afzal A, Rehman L, Javed F (2018) Impact of depressed skull fracture surgery on outcome of head injury patients. Pak J Med Sci 34: 130‐134. [Crossref]
- Aziz MM, Molla S, Abdelrahiem HA, Dawood OM (2019) Depressed Skull Fractures Overlying Dural Venous Sinuses: Management Modalities and Review of Literature. Turk Neurosurg 29: 856‐863. [Crossref]
- Elkatatny AAAM, Elreheem YAA, Hamdy T (2019) Traumatic Dural Venous Sinuses Injury. Open Access Maced J Med Sci 7: 3225‐3234. [Crossref]
- Kim YS, Jung SH, Lim DH, Kim TS, Kim JH et al. (2015) Traumatic Dural Venous Sinus Injury. Korean J Neurotrauma 11: 118‐123. [Crossref]
- Meirowsky AM (1965) Compound fractures of the convexity of the skull. Neurol Surgery Trauma Washington, D.C. Government Printing Office 604: 83-101.
- Behera SK, Senapati SB, Mishra SS, Das S (2015) Management of superior sagittal sinus injury encountered in traumatic head injury patients: Analysis of 15 cases. Asian J Neurosurg 10: 17-20. [Crossref]
- Birk DM, Tobin MK, Moss HE, Feinstein E, Charbel FT et al. (2015) Improvement in venous outflow following superior sagittal sinus decompression after a gunshot wound to the head: case report. J Neurosurg 123: 81-85. [Crossref]
- Bhatoe HS (2015) Dural venous sinus thrombosis after head injury. Neurol India 63: 832-833. [Crossref]