Tumor-Infiltrantig Lymphocytes Density as Determinant in Early Stage Colorectal Cancer Prognosis: A Single Centre Pilot Study
A B S T R A C T
Stage II colon cancer (CC) is a heterogeneous disease with different clinical behaviour. There is a high degree of uncertainty in recommending adjuvant chemotherapy, which is usually suggested in the high-risk population on the basis of TNM, stage and key biological markers. Published data suggest that specific tumor-infiltrating lymphocytes (S-TILs) (CD3+, CD8+, CD45RO+) may represent a valuable prognostic tool to drive the decision-making process.
We performed an analysis on 13 cases of stage II and III CC that relapsed, and on 15 cases that did not. We analyzed the density of CD3+, CD8+ and CD45RO+ in the surgical samples after radical surgery by IHC in the center of the tumor (CT) and in its invasive margin (IM). For each marker, we identified two grading of staining, high density (HD) or low density (LD), where the cut-off was the median value observed. This analysis was carried out stratifying patients in two cohorts: stage II (12 patients) and stage III (16 patients).
Density of CD3+, CD8+ and CD45RO+ in CT did not affect DFS and OS, except for OS in stage II pts for CD3+ (P=0.012).
Conversely HD of CD3+, CD8+ and CD45RO+ in IM showed significant benefit in DFS compared to LD (P=0.001, P=0.013 and P=0.001 respectively) in stage II patients and, only for CD3+, also in stage III patients (P=0.048). Similarly, we observed a significant gain in OS in pts with HD CD3+ and CD45RO+ (P=0.05 and P=0.003) but not CD8+ (P=0.25) in IM for stage II patients.
S-TILs might represent a valuable prognostic tool to drive the decision-making process especially for stage II CC disease, with a more pronounced role of S-TILs in IM compared to CT. Our results will be verified in ongoing large prospective study.
Keywords
Colon cancer, tumor-infiltrating lymphocytes, prognostic factor, immune contexture
Introduction
Colorectal cancer (CC) is one of the so called “big killers”. The anatomic extension of the cancer has been the principal prognostic factor. However, density, type and the place of immune cells in CC could represent a greater prognostic indicator, irrespective of the anatomic extent of the tumor. As with other solid tumors, staging is based on histopathologic criteria of tumor invasion (T), diffusion to local lymph nodes (N), distant metastases (M) and tumor cell differentiation. According to the tumor stage, the possibility of relapse is different. Therefore, the involvement of positive lymph nodes (TNM stage III) predicts a 50% to 60% possibility of relapse within 5 years, and therefore requires adjuvant chemotherapy. Stage I-II CCs have a better outcome; however, 25-30% of those patients develop a disease recurrence [1].
Surgery is the primary therapy for solid tumors. TNM stage evaluates the postoperative outcome and is useful in the decision-making process for adjuvant therapy. Since microsatellite instability (MSI) is due to disruption of the mismatch-repair system, leading to length alterations in multiple microsatellites, genes with simple repeats in their coding regions are susceptible to deletions and a high rate of mutations in MSI-H cancers [2]. These genotypes seem to influence clinical outcome [3]. Furthermore, primary tumors and metastasis expand within a microenvironment. Tumor growth may be influenced by the immune system [3, 4]. Angiogenesis is critical to the development and malignant dissemination of solid tumors through the activity of vascular endothelial growth factor (VEGF) [5, 6]. In tumor progression, cancer cells might acquire immune tolerance mechanisms by developing complex immunosuppressive networks involving interleukin (IL)-10, transforming growth factor β (TGF-β) and T cell-specific coinhibitory molecules as PD-1 and CTLA-4 [7].
In situ or T1 stage CCs (60%) are characterized by the greatest immune cell density. Conversely, T4 tumors (18%) show a higher density of tumor-infiltrating lymphocytes (TILs). TILs include T cells and B cells and mononuclear and polymorphonuclear immune cells. There are two categories of TILs: those infiltrating the stroma and those within the cancer cells. The presence of TILs is often associated with better clinical outcome [7, 8]. Mutations in DNA mismatch repair genes result in a failure to repair errors in repetitive sequences, defined as MSI. CC can be divided into three groups: MSI-H (microsatellite instability-high), MSI-L (microsatellite instability-low) and microsatellite stable (MSS). Defects in the DNA mismatch repair system are likely to cause MSI [9].
A severe lymphocytic infiltration was observed mainly in MSI-H tumors (20%), being 12.8% in MSI-L/MSS tumors [9]. MSI-H is characterized by the production of aberrant proteins that constitute ideal target for the immune system. Up to 30% of CC have evidence of a familial component and about 5% are thought to be due to well-characterized inherited mutations; although CC often occurs sporadically. Inherited syndromes such as Lynch syn¬drome (hereditary nonpolyposis colorec¬tal cancer), familial adenomatous polyposis (FAP), and MutY human homolog (MUTYH)-associated polyposis (MAP) are linked to genetic susceptibility to CC [10]. Criteria for evaluation of high-risk families include within the tumor a high MSI or abnor¬mal expression of one or more DNA mismatch repair proteins (MLH1, MSH2, MSH6, PMS2) [10]. However, conventional PCR-based MSI interrogation requires complicated steps and additional equipment, usually not available in the Pathology Departments, and shows low sensitivity for samples with a small proportion of tumor cells [11]. Thus, robust and friendly prognostic markers in CC are still an impelling need.
Mlecnik et al. studied TILs in the centre (CT) and in the invasive margin (IM) of tumors, and their data suggests that the immune contexture may affect the clinical outcome of the patients [12]. A decreased intratumoral immune T-cell density was associated with primary tumor growth and metastatic diffusion. High densities of CD8+ cytotoxic T lymphocyte infiltrate (in about 60% of patients) was related with early stage tumor (Tis/T1). There was a low correlation of the number of CD8+ cells in patients who relapsed. The density of CD8+ infiltrates was inversely correlated with T stage in patients with no recurrence. Differences in disease-free (DFS) and overall survival (OS), as evidenced by univariate analysis, was related to TILs. A Cox multivariate analysis supported its use in predicting survival and recurrence beyond TNM staging [12, 13]. TILs were a useful prognostic indicator over TNM staging and may therefore suggest to treat by adjuvant chemotherapy patients with low lymphocyte density. The immune system is unable to efficiently prevent metastatic spread. Therefore, a reduction in recurrence is due to other antitumoral immune mechanisms [13]. High density of memory T cells and Th1 seem to be a strong predictor of tumor recurrence after surgery [13]. Several studies demonstrated that high density of intratumoral FOXP3+ T regulatory cells is correlated with poor prognosis in many tumors. Nevertheless, high-density intratumoral FOXP3+ T cells in stages II and III CC are associated with an improved OS [14]. In a small study (40 CC patients), a high density of T regulatory cells was correlated with spread of disease [15]. A significant benefit in OS (P=0.0005) and PFS (P=0.0009) was demonstrated in another study of 50 patients with relapsed colorectal cancer with high intratumoral FOXP3+ T cell infiltrate [16]. Here we aimed to perform a pilot monocentric study on stage II and III CC in order to evaluate the role of TILs in CC as independent prognostic marker, over the TNM staging and irrespective of the MSI status.
Table 1: Clinical-pathological features of our cohort of CC patients, stratified for stage (II or III).
|
Stage II patients (N=12) |
Stage III patients (N=16) |
P value |
|
Age median (range) |
64.2 years (52-76.7) |
65.3 years (54.6-73.7) |
|
|
Gender |
|
|
|
|
Male |
6 |
13 |
P=0.11 |
|
Female |
6 |
3 |
|
|
Tumor size |
|
|
|
|
T1 |
0 |
0 |
P=0.56 |
|
T2 |
0 |
1 |
|
|
T3 |
10 |
11 |
|
|
T4 |
2 |
4 |
|
|
Nodal status |
|
|
|
|
N0 |
12 |
1 |
P<0.0001 |
|
N1 |
0 |
8 |
|
|
N2 |
0 |
5 |
|
|
N3 |
0 |
2 |
|
|
Grade |
|
|
|
|
G1/G2 |
9 |
11 |
P=1 |
|
G3/G4 |
3 |
5 |
|
|
Primary |
|
|
|
|
Transverse colon |
0 |
1 |
P=0.41 |
|
Left Colon |
4 |
9 |
|
|
Right colon |
3 |
3 |
|
|
Rectum |
5 |
3 |
Materials and Methods
We obtained tumor paraffin tissue from 15 cases of stage II and III CC that relapsed, and from 13 non-relapsed cases. Clinical-pathological characteristics of patients are reported in (Table 1). Patients signed a written informed consent allowing the collection and analysis of their biological material. Relapsed and non-relapsed patients were case matched for site of the primary tumor, stage, sex, age, PS and therapy. We analyzed, by IHC, CD3+, CD8+ and CD45RO+ density in the CT and in the IM of tissues collected at radical surgery. The number of positive cells per tissue surface unit (given in square millimetres) was recorded. For each antigen, we defined the median value of the observations as the cut-off for identifying high density (HD) or low density (LD) tissues. Log Rank test was used to compare DFS and OS between HD and LD patients.
Results
We reported the OS and DFS analysis in two groups of patients, stage II (12 patients) and stage III (16 patients). CD3+, CD8+ and CD45RO+ density in CT did not correlate with DFS nor OS (Figure 1, 2), with the exception of CD3+ and OS in stage II patients (P=0.012) (Figure 3). Patients with HD CD3+, CD8+ and CD45RO+ in IM presented significant longer DFS in respect to LD (P=0.001, P=0.013 and P=0.001 respectively) (Figure 4, 5) in stage II patients and, limited to CD3+, in stage III patients (P= 0.048) (Figure 6). A similar benefit was observed in OS in patients with HD CD3+ and CD45RO+ (P=0.05 and P=0.003). This was not the case of CD8+ (P=0.25) in IM for stage II patients.
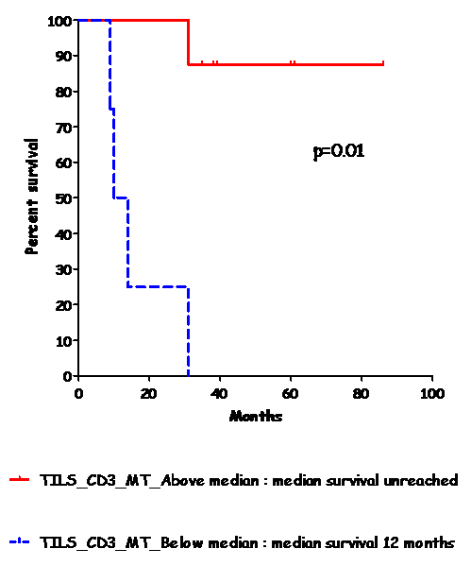
Figure 1: DFS in stage II CC patients. Kaplan-Meier curves according to CD3+ density in the margin of the tumor.
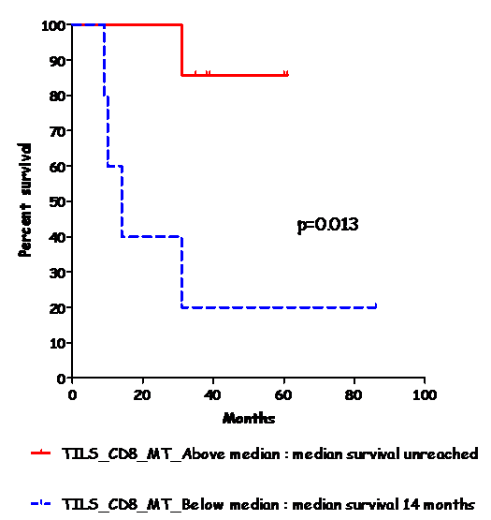
Figure 2: DFS in stage II CC patients. Kaplan-Meier curves according to CD8+ density in the margin of the tumor.
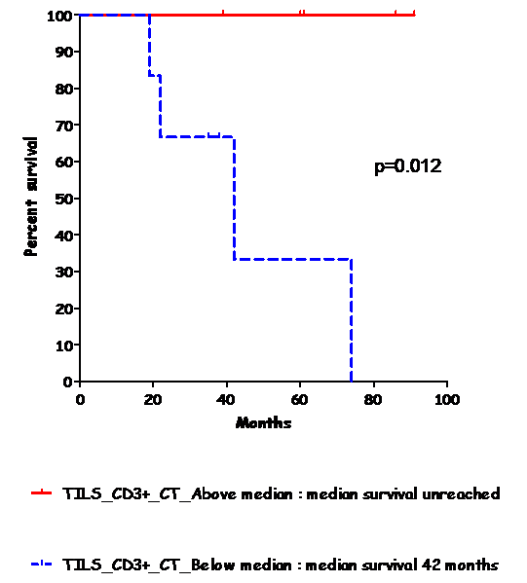
Figure 3: OS in stage II CC patients. Kaplan-Meier curves according to CD3+ density in the centre of the tumor.
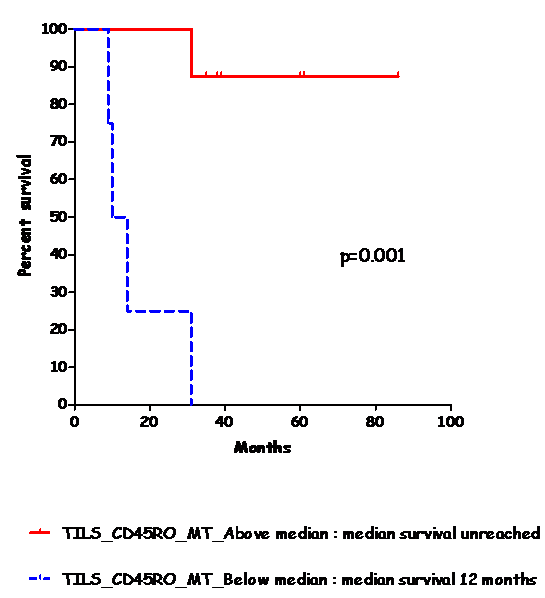
Figure 4: DFS in stage II CC patients. Kaplan-Meier curves according to CD45RO+ density in the margin of the tumor.
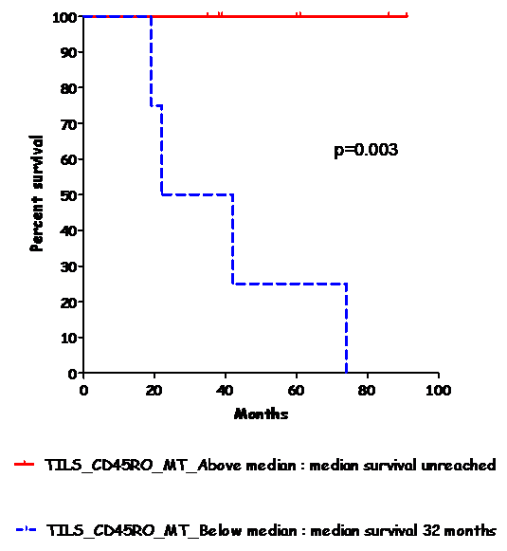
Figure 5: OS in stage II CC patients. Kaplan-Meier curves according to CD45RO+ density in the margin of the tumor.
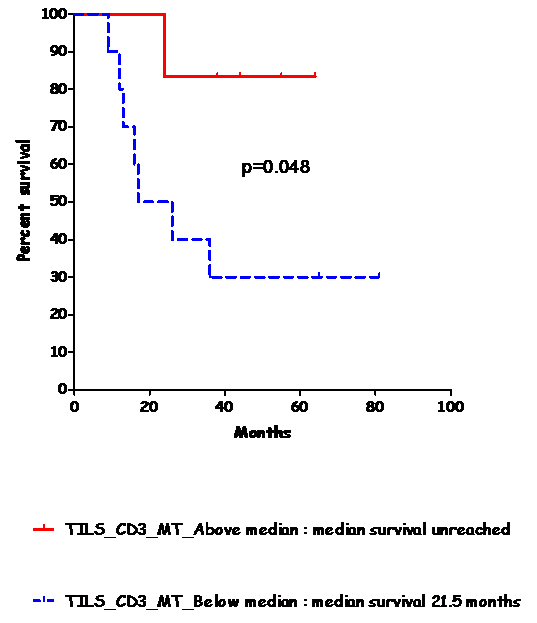
Figure 6: DFS in stage III CC patients. Kaplan-Meier curves according to CD3+ density in the margin of the tumor.
Discussion
Stage by TNM and other useful prognostic markers help the choice of adjuvant therapy in some tumors. Stage II CC is a heterogeneous disease, where advising adjuvant chemotherapy is not always easy. High and low risk stage II patients are usually defined on the basis of clinical-pathological characteristics. Adjuvant chemotherapy is routinely offered to high-risk patients. The immune system, and most importantly late-memory and cytotoxic T cells, has an anticancer effect in CC. Furthermore, effector memory T cells are able to protect, over time, growth and dissemination of micrometastases and relapse events [17]. Data from the literature indicates that specific TILs (CD3+, CD8+, CD45RO+) might provide a useful means of improving decision-making process in clinics.
In this contest, we focused on the role of TILs in CC, over the TNM staging. In particular, we investigated if TILs might have a role in determining prognosis, mainly in early stage CC. We found that density of CD3+, CD8+, CD45RO+ might represent a valuable prognostic tool to drive the decision-making process especially for stage II CC disease. This investigation, furthermore, requires IHC, which is easy to perform in any diagnostic laboratory and in the clinical setting of unselected patients. Thus, a clinically relevant translation of our pilot study is the identification of a TILs prognostic profile, based on cytotoxic and memory T cells (CD8+/CD45RO+) number, both in the CT and the IM of the lesion.
Another question is whether TILs density is associated with MSI. In fact, MSI-H tumors are characterised by a strong lymphocytic reaction [18]. Nevertheless, the majority of CC are microsatellite stable. Galon et al. investigated in primary tumors the relationship between density, type and the place of immune cells with outcome of the patients, demonstrating that the immune-classification has a superior prognostic value to the AJCC/UICC TNM-staging [19]. Immune cells are organized in graduated infiltration in the CT, at the IM and in lymph nodes adjacent to the tumor [19, 20]. In human primary solid tumours, a high density of Th1/cytotoxic memory T lymphocytes, in the CT and IM, is associated with an increased DFS and OS. This was particularly observed in CC and should be extended to most human tumors. Therefore, this classification might be useful to select high-risk patients who would receive a major benefit from adjuvant chemotherapy [21]. It has been demonstrated that MSI correlates with good prognosis [22, 23].
Guidoboni et al. showed that MSI-H tumors, with high density of TILs, show a better prognosis [17]. Camus M et al. [24] demonstrated that the coexpression of genes mediating cytotoxicity (GNLY) and Th1 adaptive immune responses (IRF1) predicted OS in CC patients independently of the metastatic spread [24, 25].
Conclusion
We here reported a pilot monocentric study on stage II and III CC, specifically aimed to evaluate the role of TILs in CC as independent prognostic marker, irrespective of MSI status. We demonstrated that TILs, more in the IM compared to the CT, might allow a more precise and personalised decision-making process in stage II CC. We are aware that the small number of patients might limit the translational value of our study. However, if confirmed by larger and independent cohorts of CC patients, this preliminary report might offer a useful prognostic tool to advice personalised therapy in early stage CCs, where there is not yet a valuable cancer-associated prognostic marker. We conclude, on the basis of our experience, that it is becoming essential to include the TILs density as a prognostic indicator, with two goals: first, as an accurate prognostic marker for DFS and OS for early stage CCs; second, as potential new target for immunotherapy and future therapeutic approaches.
Abbreviations
CC: colon cancer
TNM: tumor, nodes, metastases
S-TILs: tumor-infiltrating lymphocytes
CT: center of the tumor
IM: invasive margin of the tumor
HD: high density
LD: low density
DFS: disease free survival
OS: overall survival
MSI: microsatellite instability
MSI-H: microsatellite instability-high
MSI-L: microsatellite instability-low
MSS: microsatellite stable
VEGF: vascular endothelial growth factor
IL: interleukin
TGF-β: transforming growth factor β
PD-1: programmed Death 1
CTLA-4: Cytotoxic T-Lymphocyte Antigen 4
FAP: familiar adenomatous polyposis
MAP: MutY human homolog (MUTYH)-associated polyposis
GNLY: granulysin
IRF1: interferon regulatory factor 1
Authors Contribution
LNC and RV contributed equally to this work; LNC, RV, FT, GC and FE critically reviewed the literature on topic of this review; RV, LNC and MMC designed the pilot study; RV, GC and FE enrolled the patients and collected clinical data; FM selected patient’s tumor samples and performer IHC; VD performed the statistical analysis; all authors, equally coordinated by LNC and RV, were involved in writing of the paper and approved the final version.
Acknowledgements
We are grateful to the ARCO Foundation of Cuneo for partially supporting the pilot study.
Conflicts of Interest
The authors declare to not have any conflicting interests.
Article Info
Article Type
Research ArticlePublication history
Received: Mon 23, Sep 2019Accepted: Wed 09, Oct 2019
Published: Fri 18, Oct 2019
Copyright
© 2023 Cristiana Lo Nigro. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.RCO.2019.01.02
Figures & Tables
Table 1: Clinical-pathological features of our cohort of CC patients, stratified for stage (II or III).
|
Stage II patients (N=12) |
Stage III patients (N=16) |
P value |
|
Age median (range) |
64.2 years (52-76.7) |
65.3 years (54.6-73.7) |
|
|
Gender |
|
|
|
|
Male |
6 |
13 |
P=0.11 |
|
Female |
6 |
3 |
|
|
Tumor size |
|
|
|
|
T1 |
0 |
0 |
P=0.56 |
|
T2 |
0 |
1 |
|
|
T3 |
10 |
11 |
|
|
T4 |
2 |
4 |
|
|
Nodal status |
|
|
|
|
N0 |
12 |
1 |
P<0.0001 |
|
N1 |
0 |
8 |
|
|
N2 |
0 |
5 |
|
|
N3 |
0 |
2 |
|
|
Grade |
|
|
|
|
G1/G2 |
9 |
11 |
P=1 |
|
G3/G4 |
3 |
5 |
|
|
Primary |
|
|
|
|
Transverse colon |
0 |
1 |
P=0.41 |
|
Left Colon |
4 |
9 |
|
|
Right colon |
3 |
3 |
|
|
Rectum |
5 |
3 |
References
- Siegel R, Miller KD, Jemal A (2016) Cancer statistics, 2016 CA. Cancer J Clin 66: 7-30. [Crossref]
- Haydon AM, Jass JR (2002) Emerging pathways in colorectal-cancer development. Lancet Oncol 3: 83-88. [Crossref]
- Dunn GP, Old LJ, Schreiber RD (2004) The three Es of cancer immunoediting. Annu Rev Immunol 22: 329-360. [Crossref]
- Galon J, Fridman WH, Pages F (2007) The adaptive immunologic microenvironment in colorectal cancer: a novel perspective. Cancer Res 67: 1883-1886. [Crossref]
- Bergers G, Benjamin LE (2003) Tumorigenesis and the angiogenic switch. Nat Rev Cancer 3: 401-410. [Crossref]
- Smyth MJ, Godfrey DI, Trapani JA (2001) A fresh look at tumor immunosurveillance and immunotherapy. Nat Immunol 2: 293-299. [Crossref]
- Mocellin S, Wang E, Marincola FM (2001) Cytokines and immune response in the tumor microenvironment. J Immunother 24: 392-407. [Crossref]
- Broussard EK, Disis ML (2011) TNM staging in colorectal cancer: T is for T cell and M is for memory. J Clin Oncol 29: 601-603. [Crossref]
- Takemoto N, Konishi F, Yamashita K, Kojima M, Furukawa T et al. (2004) The correlation of microsatellite instability and tumor-infiltrating lymphocytes in hereditary non-polyposis colorectal cancer (HNPCC) and sporadic colorectal cancers: the significance of different types of lymphocyte infiltration. Jpn J Clin Oncol 34: 90-98. [Crossref]
- Provenzale D, Gupta S, Ahnen DJ, Bray T, Cannon JA et al. (2016) Genetic/Familial High Risk Assessment: Colorectal Version 1.2016, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 14: 1010-1030. [Crossref]
- Jang M, Kwon Y, Kim H, Kim H, Min BS et al. (2018) Microsatellite instability test using peptide nucleic acid probe-mediated melting point analysis: a comparison study. BMC Cancer 18: 1218. [Crossref]
- Mlecnik B, Tosolini M, Kirilovsky A, Berger A, Bindea G et al. (2011) Histopathologic-based prognostic factors of colorectal cancers are associated with the state of the local immune reaction. J Clin Oncol 29: 610-618. [Crossref]
- Mlecnik B, Bindea G, Pages F, Galon J (2011) Tumor immunosurveillance in human cancers. Cancer Metastasis Rev 30: 5-12. [Crossref]
- Salama P, Phillips M, Grieu F, Morris M, Zeps N et al. (2009) Tumor-infiltrating FOXP3+ T regulatory cells show strong prognostic significance in colorectal cancer. J Clin Oncol 27: 186-192. [Crossref]
- Loddenkemper C, Schernus M, Noutsias M, Stein H, Thiel E et al. (2006) In situ analysis of FOXP3+ regulatory T cells in human colorectal cancer. J Transl Med 4: 52. [Crossref]
- Correale P, Rotundo MS, Del Vecchio MT, Remondo C, Migali C et al. (2010) Regulatory (FoxP3+) T-cell tumor infiltration is a favorable prognostic factor in advanced colon cancer patients undergoing chemo or chemoimmunotherapy. J Immunother 33: 435-441. [Crossref]
- Guidoboni M, Gafa R, Viel A, Doglioni C, Russo A et al. (2001) Microsatellite instability and high content of activated cytotoxic lymphocytes identify colon cancer patients with a favourable prognosis. Am J Pathol 159: 297-304. [Crossref]
- Buckowitz A, Knaebel HP, Benner A, Bläker H, Gebert J et al. (2005) Microsatellite instability in colorectal cancer is associated with local lymphocyte infiltration and low frequency of distant metastases. Br J Cancer 92: 1746-1753. [Crossref]
- Galon J, Pagès F, Marincola FM, Thurin M, Trinchieri G et al. (2012) The immune score as a new possible approach for the classification of cancer. J Transl Med 10: 1. [Crossref]
- Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A, Mlecnik B et al. (2006) Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science 313: 1960-1964. [Crossref]
- Pages F, Galon J, Dieu-Nosjean MC, Tartour E, Sautès-Fridman C et al. (2010) Immune infiltration in human tumors: a prognostic factor that should not be ignored. Oncogene 29: 1093-1102. [Crossref]
- Popat S, Houlston RS (2005) A systematic review and meta-analysis of the relationship between chromosome 18q genotype, DCC status and colorectal cancer prognosis. Eur J Cancer 41: 2060-2070. [Crossref]
- Schwitalle Y, Kloor M, Eiermann S, Linnebacher M, Kienle P et al. (2008) Immune response against frameshift-induced neopeptides in HNPCC patients and healthy HNPCC mutation carriers. Gastroenterology 134: 988-997. [Crossref]
- Camus M, Tosolini M, Mlecnik B, Pagès F, Kirilovsky A et al. (2009) Coordination of intratumoral immune reaction and human colorectal cancer recurrence. Cancer Res 69: 2685-2693. [Crossref]
- Saeterdal I, Bjorheim J, Lislerud K, Gjertsen MK, Bukholm IK et al. (2001) Frameshift-mutation-derived peptides as tumor-specific antigens in inherited and spontaneous colorectal cancer. Proc Natl Acad Sci USA 98: 13255-13260. [Crossref]