Complicated Spigelian Hernia with Incarcerated Appendicitis Presenting as a Local Cellulitis
A B S T R A C T
We discuss here the case of a unique case of a complicated Spigelian hernia with incarcerated appendicitis presenting with a local cellulitis in the general emergency unit of a French hospital. Here, a local approach was performed and the appendicitis was operated on the site of the observed cellulitis, allowing the surgeon to take care of both the cellulitis, appendicitis and hernia.
Keywords
Appendicitis, complicated Spigelian hernia, cellulitis
Introduction
Appendicitis is one of the most common causes of abdominal pain. Spigelian hernia is a rare abdominal wall deficiency, consisting of a lateral ventral hernia, along the semilunar line. Those two conditions may coexist and lead to unusual clinical presentation. This case report aims at showing the management of a possible complication of such a situation that occurred in a teaching hospital in France.
Case Presentation
We introduce the interesting case of an 87-year-old patient who was admitted in the general adult emergency unit for abdominal pain, which lasted for two days, located in the right iliac fossa. His medical history included a chronic respiratory insufficiency caused by a chronic obstructive pulmonary disease associated with tobacco smoking with emphysema, essential hypertension, and a Lichtenstein tension-free left inguinal hernia repair.
He reported no nausea, vomiting, diarrhea or constipation. He was admitted with a local inflammation with erythema and tenderness of the skin in the right iliac fossa, suggesting cellulitis, with an elevated body temperature up to 38.4°C without shivers. Abdominal palpation revealed a right iliac fossa guarding. The blood sampling results showed an inflammation with leukocytosis up to 18*10/9 G/L and a CRP level of 200 mg/L. The CT scan imaging, showed in (Figure 1) described a Spigelian hernia included appendicitis in the right iliac fossa associated with local cellulitis, without any digestive perforation sign.
Thus, the patient, his vital signs remaining stable, was addressed to the emergency general surgical team and the surgery consisted in an appendicectomy via elective abdominal section resembling the Mc Burney section, a repair by suturing of the hernia and both intra-abdominal (with a Blake drainer) and subcutaneous drainage was performed during the hospital stay.
The intra operative observation concluded in an appendicitis trapped in an anterior abdominal wall hernia with a hernial sac moving the transverse abdominal muscle fibers apart. Photos in (Figure 2) show the intra-operative dissection with the oedematous and inflammatory appendix after opening the abdominal wall.
Postoperatively, the patient’s medical condition improved quickly, even though he required a short stay in intensive care due to his medical respiratory terrain. A short antibiotherapy was given for 6 days. The surgical site required white dressing changes twice a day and the use of a hemostatic mesh. The control blood sampling showed regression of the inflammatory patterns, and the patient was discharged after a week of hospital stay.
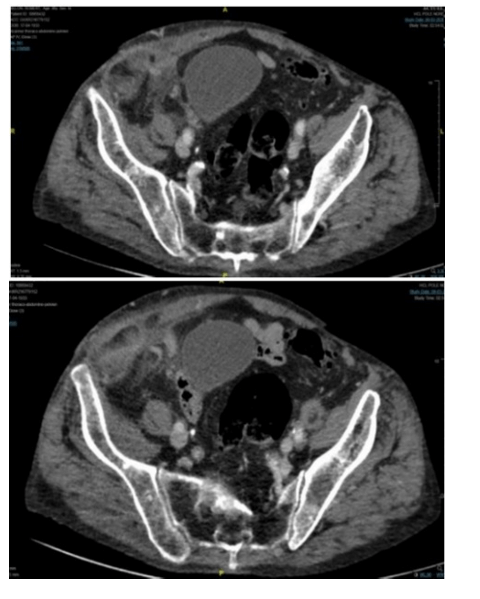
Figure 1: Injected CT Scan.

Figure 2: A) View after dissection. B) View after mesoappendix dissection.
Discussion
A review of the literature found some cases of extra-abdominal appendicitis. Those were mostly related to other diagnoses, with abdominal wall deficiency, as Amyand’s hernia (appendix incarcerated in an inguinal hernia) and De Garengeot’s hernia (incarcerated femoral hernia). Exceptional cases of paraumbilical hernia with incarcerated appendix are also reported. But when it comes to Spigelian hernias, the number of incarcerated appendicitis cases reported decreases.
Few cases of abdominal wall cellulitis were reported [1-3]. The first one, written by Yamaguchi et al., concerning a neurologically disabled patient, did not report the surgical technique but emphasized the importance of being aware of such cases and cautious with patients suffering from communication troubles. The second one, by Ahmed K et al., also reports an abdominal abscess but secondary to an Amyand’s hernia, which was treated by open appendicectomy. The third one, reported by Beerle C et al., was unique regarding by its surgical strategy, as the hernia reparation was performed by coelioscopy and by the use of an omental patch to cover the abdominal wall defect.
Appendicitis may be a misleading diagnosis, due to anatomical variations, symptoms differences, and initial motivation for urgent consulting. With associated lesions, it may even present with atypical clinical signs, which should encourage emergency doctors to keep cautious and alert towards unusual features. Abdominal wall cellulitis should be first evaluated by imaging, as it is hard to make a clear and reliable etiological diagnosis based on clinical signs only.
This case is unique as it illustrates a direct approach of treating appendicitis through the parietal complication and starting the operation on the infected site. We hope to keep readers aware and curious about clinical mismatch and unusual clinical presentations of appendicitis.
Article Info
Article Type
Case ReportPublication history
Received: Sat 23, May 2020Accepted: Thu 11, Jun 2020
Published: Tue 23, Jun 2020
Copyright
© 2023 O. Monneuse. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.06.17
Figures & Tables
References
- Hiroyuki Yamaguchi, Hiroyuki Kobayashi, Kazuya Nagasaki (2020) Abdominal Wall Cellulitis in Acute Abdomen. Intern Med 59: 595. [Crossref]
- Khalid Ahmed, Suhail Hakim, Ahmed M. Suliman, Ammar Aleter, Ayman El-Menyar et al. (2017) Acute appendicitis presenting as an abdominal wall abscess: A case report. Int J Surg Case Rep 35: 37-40. [Crossref]
- Corinne Beerle, Hans Gelpke, Stefan Breitenstein, Ralph F Staerkle (2016) Complicated acute appendicitis presenting as a rapidly progressive soft tissue infection of the abdominal wall: a case report. J Med Case Rep 10: 331. [Crossref]